
2.3.3 The Subcostal Window
The subcostal window has many advantages. There is no bone or lung tissue to obstruct our view to the heart. The subcostal window permits us to image patients in supine position. Once you are familiar with the subcostal window you will see that it is not only a substitute for the parasternal and the apical window, but that it is quite superior to these windows. In addition, some pathologies can only be investigated from the subcostal approach.
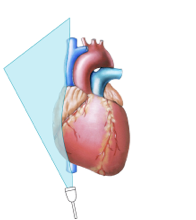
Specific indications for the subcostal window The patient cannot be positioned on his/her left side Poor quality of the parasternal and/or apical image COPD Imaging from other windows is not possible (surgical or other scars of the chest) Malposition of the heart Make the subcostal window an integral part of every exam.To image from the subcostal window the patient should lie supine. Patients with tense abdominal muscles should be asked to bend their knees. Place the transducer under the xiphoid, slightly to the right of the sternum. The transducer marker should be to the left; the imaging plane should be directed upwards and to the left shoulder in slightly clockwise rotation. Ask the patient to inhale while you advance the transducer towards the heart. Inspiration fills the lungs and displaces the diaphragm and the liver caudally. This allows the heart to move closer to the transducer. As is true for other windows, a large number of cut planes can be derived from the subcostal window.
2.3.3.1 Subcostal Four-Chamber View
Start with the subcostal four-chamber view. This is the view you will obtain when the marker is to the left. It looks very similar to the four-chamber view, with the difference that the apex is more to the left, the septum is oblique, and the right heart chambers are in the near field right below the liver.
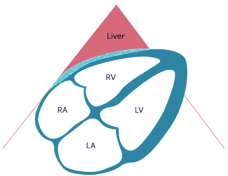
As on the four-chamber view, you will be able to assess the chambers of the heart, especially the right ventricle. Besides, this view is ideal to visualize a pericardial effusion, which is often found adjacent to the right heart. As you are imaging the interatrial septum in perpendicular fashion, you can also identify atrial septal defects on this view.
You can see a right-sided pleural effusion on the subcostal four-chamber view.2.3.3.2 Subcostal Short-Axis View
By rotating the transducer counterclockwise you can create short-axis views. Short-axis views can be obtained at different levels by moving the transducer more to the left to view the ventricular segments, and to the right to view the basal segments. These views are very similar to the short-axis views you obtain from a parasternal approach.
Subcostal SAX Base Subcostal SAX LV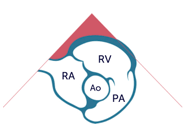
 Video Platform Video Management Video Solutions Video Player
Video Platform Video Management Video Solutions Video Player
Subcostal short axis view
Video Platform Video Management Video Solutions Video Player
Video Platform Video Management Video Solutions Video Player
Subcostal short axis view
In some patients you can even perform M-Mode measurements of the left ventricle. On the short axis view at the base you will be able to see the pulmonary valve and the pulmonary artery. Thus, this view serves as an alternative to the parasternal view of the pulmonary trunk, which may be difficult to obtain in some patients.
2.3.3.3 Subcostal Vena Cava View
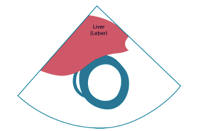
The easiest way to obtain the subcostal view of the inferior vena cava is to start with a four-chamber view. Make sure the right atrium is in the center of the image. Then rotate the transducer counterclockwise and direct it to the right. The subcostal view shows the vena cava inferior in a "long axis". The axis of the transducer is parallel to the cranio-caudal axis of the body.
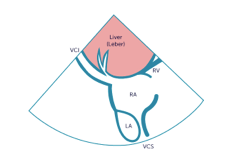
On this view you will not only see the inferior vena cava as it enters the right atrium, but also the hepatic veins which drain into the inferior vena cava below the diaphragm. In some patients it may even be possible to view the superior vena cava in the far field of the image. This view has numerous uses: in addition to assessing the size and blood flow of the inferior vena cava and the hepatic veins, you can identify a prominent Eustachian valve, a pericardial effusion, or a (right-sided) pleural effusion.
Specific uses of the subcostal VCI view Assessing the size and blood flow of the inferior vena cava and the hepatic veins Pericardial effusion Assessing signs of tamponade Pleural effusion (right sided) The Eustachian valve is clearly seen Follow the respiratory movements of the abdomen when you assess the width of the inferior vena cava. Remember that the width of the vena cava decreases with inspiration.