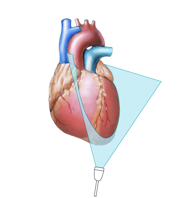
2.3.2 Apical Window
The apical window is the second window from which you should image. The patient is again positioned on his/her left side, but not as far as is the case when using the parasternal window. The apical window is usually found in the fifth intercostal space but again, the patient's constitution largely determines the position of the apex. In slim or asthenic patents it is more medial - in the region of the anterior axillary line. However, in obese patients and in those with a pyknic constitution the apex may be much further lateral and sometimes even dorsal. You will be able to determine the position of the apex by feeling the apical impulse.
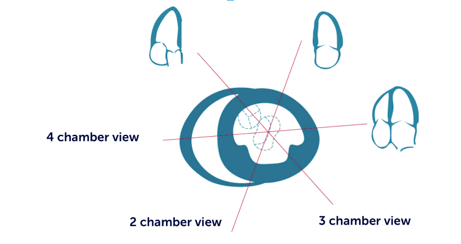
2.3.2.1 Four-Chamber View
The four-chamber view is probably the most important view in echocardiography. If you get lost, always go back to the four-chamber view.
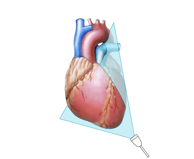
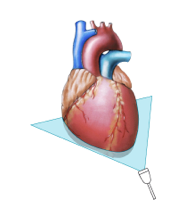
For this view the marker of the transducer is positioned to the left and the image plane is oriented cranially towards the head. The heart is cut similar to the way you would cut a bread roll.

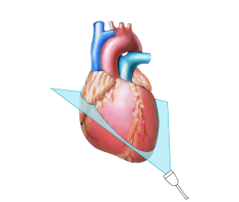 The four-chamber view „cuts“ the heart like a „bread role“
Cut plane of the four-chamber view
The four-chamber view „cuts“ the heart like a „bread role“
Cut plane of the four-chamber view
The leading structure is the interventricular septum, which should be displayed such that it is parallel to the ultrasound beam. This is done by moving the transducer either medially or laterally.
This view demonstrates all four chambers of the heart. Here we see the lateral and septal myocardial segments. A more detailed description of myocardial segments can be found in Chapter 8, Coronary Artery Disease. On the four-chamber view you will almost never really transect the heart at its true apex. This phenomenon is known as foreshortening. To help you see more of the apex you need to use modified views.
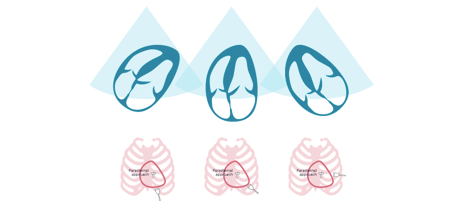
You can easily miss pathologies of the apex such as a supraapical infarction or a thrombus due to foreshortening - Use atypical views that help you to see more of the apex. Video Platform Video Management Video Solutions Video Player Four-chamber view without foreshortening Video Platform Video Management Video Solutions Video Player Four-chamber view with foreshortening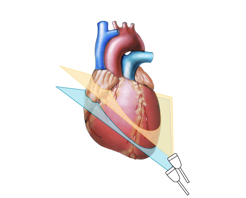
 Cut planes of the four-chamber view with and without foreshortening
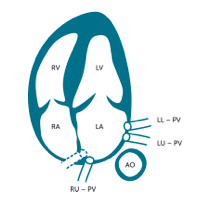
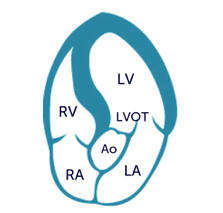
Structures seen on the apical four-chamber view
Cut planes of the four-chamber view with and without foreshortening
Structures seen on the apical four-chamber view
Other visible structures are the mitral and tricuspid valve, the pulmonary veins, the interatrial septum and the descending aorta. The four-chamber view is ideal to assess contractile function, study the heart valves, and several other aspects of the heart. You simply cannot perform a conclusive study without a four-chamber view.
2.3.2.2 Two-Chamber View
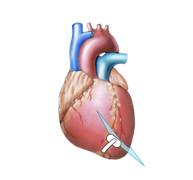
By rotating the transducer approximately 60 degrees in counterclockwise direction you obtain the two-chamber view.
Before you rotate make sure that the center line of the image passes through the center of the left ventricle and the left atrium is displayed in its full length. When rotating the transducer you should not alter your angulation or lose your position. The two-chamber view displays the left ventricle and the left atrium. You should not see the interventricular septum.
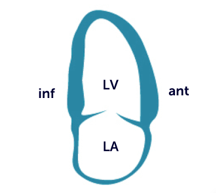
Apart from the fact that you can view different segments of the heart (anterior and inferior wall), there is also less foreshortening of the apex on the two-chamber view. You will be able to see the coronary sinus which is cut orthogonally, and the descending aorta (usually in more or less longitudinal orientation). The two-chamber view is an integral part of the echo exam because it enables you to detect abnormalities in regional wall motion in the visible segments, as well as estimate global left-ventricular function. As you will see in Chapter 12 (Mitral Regurgitation), it should also be used to evaluate the mitral valve.
2.3.2.3 Three-Chamber View
You obtain the three-chamber view by rotating the transducer even further in counterclockwise direction from the two-chamber view (approximately a further 60°).
The three-chamber view (also known as the apical long-axis view) looks very similar to the parasternal long axis. After all we are using almost the same cut plane. The only difference is that we are now imaging the heart from the apex. Therefore the apex is also seen (as opposed to the parasternal long axis). The three-chamber view displays different segments of the left ventricle (anterior septum and posterolateral segments). In addition, you can see the left ventricular outflow tract (LVOT), the left atrium, and the aortic valve.
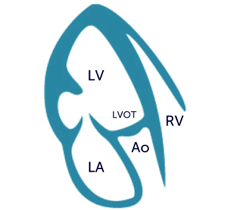
In contrast to the parasternal long axis the LVOT is now more parallel to the insonation angle. Therefore this view is ideal to study flow in the LVOT (i.e. aortic regurgitation).
2.3.2.4 Five-Chamber View (5ch View)
To obtain the five-chamber view you need to start with a four-chamber view. However, in contrast to the above mentioned views we do not rotate the transducer, but "tilt" it ventrally.
Actually, in order to obtain a good five-chamber view you should move the transducer further laterally so that the septum is in oblique position. On the five-chamber view you will be able to see the LVOT and the aortic valve, which is positioned closer to the chest. You will still see the left and right ventricle, and at least parts of the atria. In the context of echocardiography we refer to the LVOT as the fifth chamber.
The five-chamber view is mainly used to assess the aortic valve (stenosis and regurgitation) and study pathologies of the LVOT. In addition, it reveals various portions of the myocardium and the mitral valve (anterolateral commissural region).
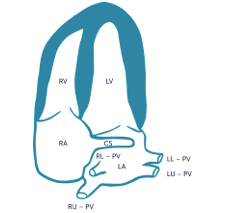
2.3.2.5 Coronary Sinus View (CS View)
The coronary sinus view has not really been "defined" as a standard view but still is an important adjunct to the other apical views because it demonstrates structures that are not seen as clearly elsewhere. For the coronary sinus view you tilt the transducer dorsally. Basically you move the transducer in the opposite direction as you would for the five-chamber view.
Here you transect the heart at its lower end. You will see the basal segments of the left ventricle and especially the basal portions of the interventricular septum. The main advantage of the CS view is that one can inspect the coronary sinus (which runs in the coronary sulcus between the ventricles and the atria) as it enters the right atrium. The CS view is also ideal to study the posteromedial commissure of the mitral valve.
2.3.2.6 Atypical Lateral View
Another "modified" view which is quite informative is the "atypical lateral view". Again, start with a four-chamber view. Rotate the transducer clockwise by about 30 to 40°. You rotate in the exactly opposite direction as you would to obtain the two-chamber view. You will eventually see the LVOT and the aortic valve. Actually this view is similar to the 5-chamber view. However, you visualize different segments of the left ventricular myocardium and see the LVOT/aortic valve in a slightly different plane. You can also identify abnormalities of wall motion in the high lateral region. In addition, it is ideal to visualize eccentric aortic regurgitation jets.

The following graphic chart shows the interrelationship between rotational apical views and short-axis views. In combination with the five-chamber view, the coronary sinus view and the atypical lateral view, the atypical lateral view permits you to scan the entire heart.