
12.3 Hemodynamics of mitral regurgitation
Mitral regurgitation overloads the volume of the left ventricle as well as the left atrium. The left ventricle has to cope with stroke volume and regurgitant volume. The way the ventricle reacts depends not only on the severity of regurgitation, but also on how rapidly regurgitation develops and how long it persists. Basically the ventricle can adapt in three ways, i.e. by increasing its:
- size,
- contractility, or
- heart rate.
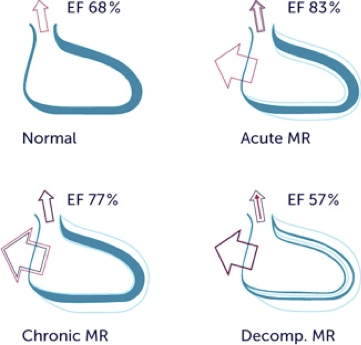
Usually all of these mechanisms are involved. However, in the setting of acute mitral regurgitation the ventricle is unable to increase its size rapidly. Thus, the ventricle has to rely on the other two mechanisms to maintain adequate stroke volume. Therefore, acute mitral regurgitation is characterized by a hyperdynamic, rapidly beating left ventricle that is either is normal or slightly enlarged.
Signs of acute MR Hyperdynamic LV normal size Tachycardia 2D morphology (visible defect) Low velocity (shock) Triangular MR - spectrum Elevated MV - inflow velocity Acute MR may be difficult to diagnose, because patients have low velocity MR jets (shock), tachycardia and tachypnea. Acute MR following leaflet rupture after valvuloplasty. Note the small hyperdynamic left ventricle.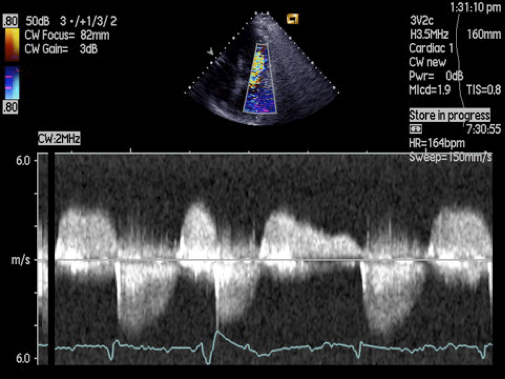
In chronic mitral regurgitation the left ventricle dilates gradually. Left ventricular function is still above normal. In this stage the ventricle is able to compensate. The ventricle is able to cope with severe mitral regurgitation for long periods (even decades). However, eventually the ventricle will fail. This condition is referred to as "decompensated mitral regurgitation". At this point the ventricle dilates further and ejection fraction begins to drop - first to so-called normal values (50-60%) and then below normal.
It should be noted that mitral regurgitation is marked by a state of decreased afterload (unloaded left ventricle). The ventricle pumps against less resistance and blood is able to "escape" through the defect. A rough analogy would be the fact that one needs to press a bicycle pump less strenuously when there is a hole in the tubing. Left ventricular function appears "better" than it is, and drops after mitral valve surgery (see section titled Treatments strategies in mitral regurgitation).
Higher afterload (i.e. hypertension) may aggravate the degree of mitral regurgitationDilatation of the ventricle causes annular dilatation which, in turn, increases mitral regurgitation. Severe mitral regurgitation is therefore not a benign condition. Patients must be monitored closely to prevent irreversible damage to the ventricle.
In a setting of significant MR, an ejection fraction of 55% to 60% (which is otherwise considered normal) already denotes left ventricular failure. Natural history of severe MR The 10-year survival rate is 57% The 5-year all-cause mortality in asymptomatic MR patients is 22% The 5-year risk for cardiac events in asymptomatic MR patients is 33% Severe MR is no benign condition.Regurgitation of blood into the left atrium increases the size of the left atrium. In compensated stages of mitral regurgitation, left atrial pressure may still be normal or just mildly elevated. However, once the ventricle starts to fail, left atrial pressure, capillary wedge pressure and pulmonary artery pressures rise. Pulmonary hypertension may lead to right heart dilatation and tricuspid regurgitation. All of these abnormalities can be seen with echo and should be taken into account when assessing the hemodynamic sequelae of mitral regurgitation.
Findings and consequences of mitral regurgitation Volume overload (dilated hyperdynamic LV) Reduced systolic wall stress Decreased afterload (unloaded left ventricle) Elevated LA + pulmonary capillary wedge pressure Left atrial enlargement Annular dilatation (more MR) Pulmonary hypertension (Tricuspid regurgitation) (Right heart failure)