
Uncomplicated acute calculous cholecystitis
Case Presentation
A 40 year old woman presents with acute pain in the right upper quadrant of 3 hours duration. The pain radiates to her shoulder with associated nausea.
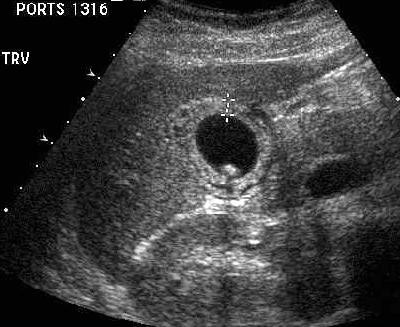 Caption: Transverse view of the gallbladder. | Description: Transverse scan demonstrating a thickened gallbladder wall, with cholelithiasis. The gallbladder wall shows alternate hypo and hyperechoic layers. The patient was very tender while scanning.
Caption: Transverse view of the gallbladder. | Description: Transverse scan demonstrating a thickened gallbladder wall, with cholelithiasis. The gallbladder wall shows alternate hypo and hyperechoic layers. The patient was very tender while scanning.
First published on SonoWorld
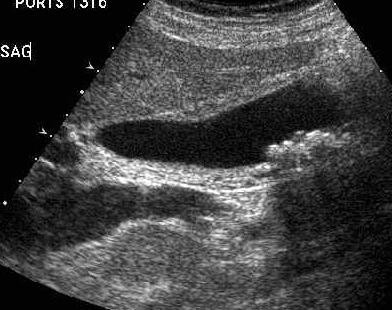 Caption: Sagittal view of the gallbladder. | Description: Sagittal scan demonstrating a distended gallbladder with multiple, mobile calculi that shadow. The gallbladder wall is significantly thickened. No pericholecystic fluid is seen.
Caption: Sagittal view of the gallbladder. | Description: Sagittal scan demonstrating a distended gallbladder with multiple, mobile calculi that shadow. The gallbladder wall is significantly thickened. No pericholecystic fluid is seen.
 Caption: Transverse scan of the gallbladder. | Description: Transverse view showing the laminated appearance of the gallbladder wall.
Caption: Transverse scan of the gallbladder. | Description: Transverse view showing the laminated appearance of the gallbladder wall.
 Caption: Color Doppler view of the gallbladder. | Description: Hyperemia of the gallbladder wall is demonstrated.
Caption: Color Doppler view of the gallbladder. | Description: Hyperemia of the gallbladder wall is demonstrated.
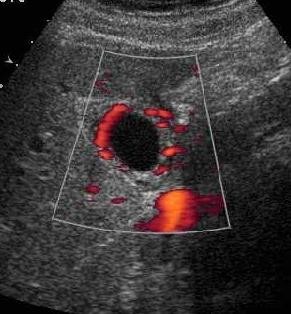 Caption: Power Doppler scan. | Description: Power Doppler view demonstrating the increased vascularity of the gallbladder wall.
Caption: Power Doppler scan. | Description: Power Doppler view demonstrating the increased vascularity of the gallbladder wall.
Differential Diagnosis
Acute cholecystitis with cholelithiasis.
Final Diagnosis
Acute cholecystitis with cholelithiasis.
Discussion
Acute cholecystitis is a common abdominal inflammatory pathology, which if undiagnosed is the cause of many mortalities and morbidities. The complications of an acutely inflamed gallbladder include rupture, peritonitis, abscess formation, and conversion to emphysematous or gangrenous form.
Ultrasound is the imaging modality to diagnose inflammatory pathologies of the gallbladder, acute or chronic. Literature has described certain ultrasound signs that point to an acute inflammatory pathology of the gallbladder. These include gallbladder distension, wall thickening (> 3mm), gallbladder wall anechogenecity, intraluminal echoes, positive sonographic Murphy’s sign [which is maximal tenderness elicited over a sonographically localized gallbladder], pericholecystic fluid, and calculi. Although not totally specific, the presence of even 2 findings combined with clinical suspicion, may be adequate to make the diagnosis of acute cholecystitis. Focal tenderness over the gallbladder while scanning is very specific for acute cholecystitis, and should always be looked for.
Wall thickening is not specific for cholecystitis, and has numerous causes. The finding of striated wall thickening, consisting of alternating layers of hypoechoic and hyperechoic bands has been reported as an indicator of acute cholecystitis. The anechoic layers have been shown to correspond pathologically to a complex of edema, hemorrhage and inflammatory cell infiltrate. However, this ultrasound finding is also nonspecific, and can be seen in the setting of congestive heart failure, renal failure, liver disease and hypoalbuminemia among other causes. In the setting of acute cholecystitis, this finding has been shown to correlate pathologically with gangrenous changes in the wall. A uniformly hypoechoic gallbladder wall may be due to changes caused by severe inflammation and subsequent sloughing of the mucosa. A small contracted gallbladder with thickened walls is more likely to be chronic cholecystitis. Cholelithiasis can be a feature of both.
The presence of perforation may be inferred from the findings of free peritoneal fluid, pericholecystic fluid collections and disappearance of the gallbladder wall echoes. Emphysematous cholecystitis would show echogenic foci within the gallbladder wall, with dirty posterior shadowing and is seen more commonly in diabetics.
Color Doppler imaging is a useful adjunct in cases of acute cholecystitis, with studies proving it to be more specific than gray-scale imaging alone. Demonstration of a hyperemic gallbladder wall [especially in the mid and fundal wall] favors more the possibility of an acute pathology. Power Doppler may be more sensitive in detecting the flow within the wall. However patients with necrotizing acute cholecystitis may show no color flow in their walls.
Radionuclide imaging can be very helpful to distinguish acute cholecystitis from choledocholithiasis and to confirm cholecystitis in equivocal cases.
Case References
1. Pinto A, et al. Personal experience in 71 consecutive patients with acute cholecystitis. Radiol Med (Torino). 2000; 99(1-2):62-7.
2. Paivansalo M, et al. Ultrasound in acute and chronic cholecystitis. Rofo Forts Geb Rontgen Nuklearmed. 1987; 147(1):84-7.
3. Soiva M, et al. Ultrasonography of the gallbladder in patients with a clinical suspicion of acute cholecystitis. Diagn Imaging Clin Med. 1986;55(6):337-42.
4. Cohan RH, et al. Striated intramural gallbladder lucencies on US studies: predictors of acute cholecystitis. Radiology. 1987; 164(1):31-5.
5. Schiller VL, et al. Color Doppler imaging of the gallbladder wall in acute cholecystitis: sono-pathologic correlation. Abdom Imaging. 1996; 21(3):233-7.
6. Draghi F, et al. Power Doppler ultrasound of gallbladder wall vascularization in inflammation: clinical implications. Eur Radiol. 2000; 10(10):1587-90.
7. Laing FC, et al. Ultrasonic evaluation of patients with acute ruq pain. Radiology. 1981: 140(2):449-55.