
2.3.2 Parasternal short-axis views



By rotating the transducer 90 degrees from PLAX in a clockwise direction you will obtain a parasternal short-axis (PSAX) view. We define several short-axis views, each cutting the heart at a different level between the base and the apex. The entire heart can be scanned using these short-axis views.
When you rotate the transducer, the rotational axis is the mid-line of the sector. Adjust the transducer so that the structure(s) you want to image in the short-axis view is/are in the center of your image.
Cut planes of the parasternal short-axis views
2.3.2.1 Parasternal short-axis - base (PSAX Base)
This view demonstrates the cranial portions of the heart. It is important to adjust the image so that the aortic root is seen as a round structure, with all three aortic valve cusps visible.
The appearance of the aortic valve during diastole resembles that of a "Mercedes star".
Orientation of the aortic valve cusps: the right coronary cusp is close to the RVOT, the left coronary cusp is close to the pulmonary artery, and the acoronary cusp is close to the interatrial septum.

Orientation of the aortic valve cusps: the right coronary cusp is close to the RVOT, the left coronary cusp is close to the pulmonary artery, and the acoronary cusp is close to the interatrial septum
Given a good quality of the image, you will be able to visualize the origins of the coronary artery, especially that of the right coronary artery.
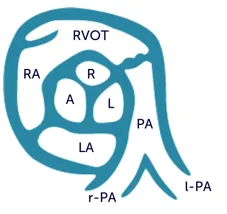
The aorta is in the center of the image, and starting at the bottom and moving in a clockwise direction, is surrounded by the left atrium, the interatrial septum, the right atrium, the right ventricle, and the pulmonary artery. You can see all the cusps of the aortic valve in this view, therefore it is ideal to observe the opening and closing motion of the valve. This view also enables you to estimate the size of the left atrium and detect atrial septal defects (ASD), although it is not ideal for this purpose - in most cases, you will have to use an atypical short-axis view from one or two intercostal spaces further down in order to detect ASDs. The PSAX base view should also be used to study the tricuspid valve and to identify any membranous ventricular septal defect, pathologies of the right ventricular outflow tract (RVOT), or the pulmonary valve (PV). You can use a modification of the PSAX base view to assess the PV and the pulmonary artery: just direct the transducer more to the left and tilt it ventrally. Sometimes it may be necessary to move to a lower intercostal space to obtain the image, where it is possible to see the bifurcation of the pulmonary artery and its branches. The right pulmonary artery is visualized here as it passes beneath the aortic arch. This view will also permit you to detect a patent ductus arteriosus (PDA).
Visualization of the PA using a modified parasternal short-axis view

2.3.2.2 Parasternal short-axis - mitral valve (PSAX-MV)
By tilting the transducer towards the apex of the LV but staying perpendicular to the long axis of the heart, you will first arrive at the plane of the mitral valve. Here the mitral valve is seen orthogonally with its anterior and its posterior leaflet. This view is ideal to observe the opening and closing motion of the mitral valve, which has been compared to a moving fishmouth.

Systole

Diastole
The motion of the mitral valve in the parasternal short-axis view resembles a fishmouth.
Parasternal short-axis view at the level of the mitral valve
Above the mitral valve, we can see the left ventricular outflow tract (LVOT). The left ventricle is surrounded by the half-moon-shaped right ventricle, the portion of the myocardium between the LV and RV is known as the interventricular septum. This view is mainly used to assess the morphology and function of the mitral valve - it is possible to observe the extent of mitral annular calcification, the size of the mitral orifice in mitral stenosis, and the origin of mitral regurgitation (with color Doppler) here.
The PSAX base view should not be used to assess LVF, since we are too near to the base of the ventricle here and the segments are thus not representative.
2.3.2.3 Parasternal short-axis - left ventricle - base (PSAX LV)
If you tilt the transducer further towards the apex you will "loose" the mitral valve and cut the heart at the base of the left ventricle.
While tilting, make sure that the left ventricle stays round - if the left ventricle becomes oval you should move up one or two intercostal spaces. In this view, you will be able to see the chordae of the mitral valve (you are not at the level of the papillary muscle yet), and the basal segments of the left and right ventricle.
Parasternal short axis at the level of the left ventricular base
This is where you should perform M-Mode measurements of the left ventricle. This view is also useful to assess the size and radial function (regional and global) of the left ventricle on the 2D image. Here you will be able to see abnormalities of the interventricular septum and estimate left ventricular size and function.
2.3.2.4 Parasternal short-axis mid-ventricle (PSAX LV-Mid)
By tilting the transducer even further towards the apex you will gradually see the papillary muscles appearing. Now you are transecting the left ventricle almost through the middle, the papillary muscle may vary in terms of size and position here. The right ventricle can also be seen but is more narrow here than on the PSAX LV base view.
The PSAX LV-Mid view is ideal to inspect features such as left ventricular function (regional and global), the size of the ventricles, and characteristics of left ventricular hypertrophy.
Parasternal short-axis at the level of the „mid ventricle“
2.3.2.5 Parasternal short-axis - apex
To view the apical segments of the ventricle from the parasternal window you need to move the transducer down by one or two intercostal spaces and tilt it towards the apex. The transducer position is quite far from the apex when we visualize from the parasternal window, so we have to get closer to it. Actually, the best point of view is halfway between the second parasternal short-axis view and the apex. The left ventricle appears much smaller in this view because we cut the left ventricle close to the apex, where its diameter is small. This view is not really a standard view but is very helpful in many situations, such as when assessing apical left ventricular function or identifying an apical thrombus.