
3.2 The left ventricle
3.2.1 Shape of the left ventricle
The shape of the left ventricular cavity has been compared to that of a bullet (prolate ellipsoid).

Of course not all "normal" ventricles have exactly the same appearance. The shape of the ventricle is influenced by the patient's habitus (physiognomy), the configuration of the chest, and many other factors. However, a grossly abnormal geometry of a ventricle may indicate the presence of a pathology. In dilated cardiomyopathy, for instance, the ventricle tends to be more spherical. In apical hypertrophic cardiomyopathy the cavity resembles the "spades" sign. In stress cardiomyopathy or left ventricular aneurysms, the apex is widened.
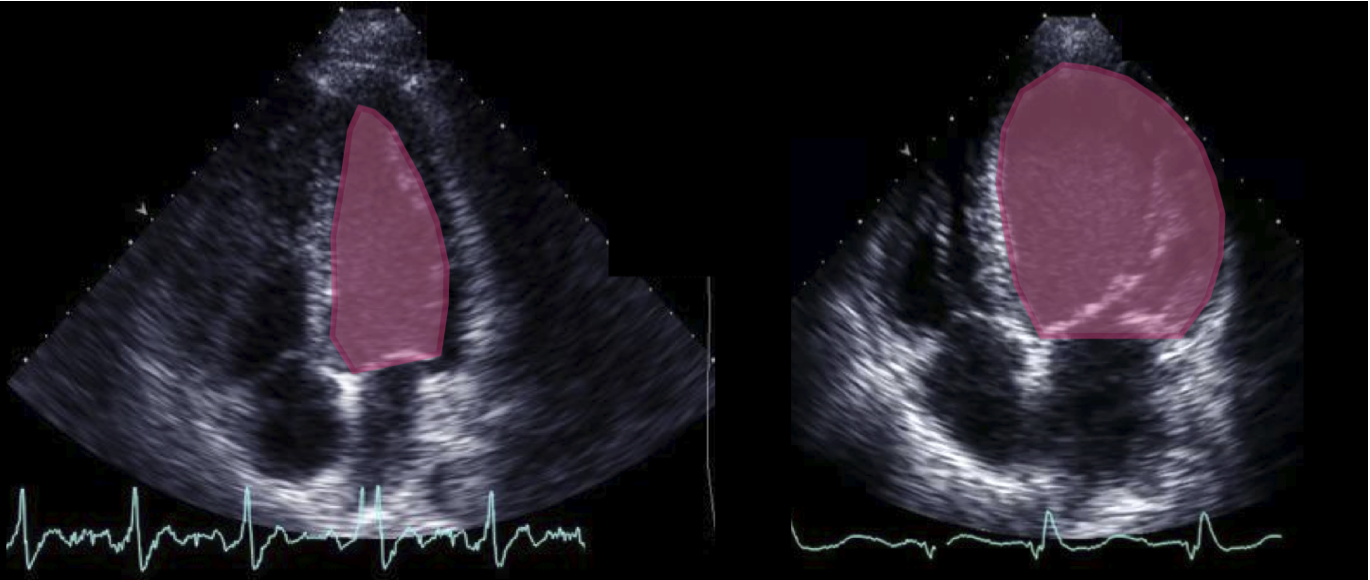
In stress cardiomyopathy, apical dilatation may be very pronounced. This entity has been termed "apical ballooning" or the "Tako-Tsubo syndrome" (you will read more about this pathology in Chapter 5).The geometry of the left ventricle is also important for the function of the heart. We now know that distortion of the ventricles alters the architecture (fiber orientation) of the myocardium. This affects the function of the ventricle as well. Geometric abnormalities lead to abnormal blood flow patterns (disturbance of normal vortex flow), which is important for the propagation and energy conservation of flow. Remodeling of the ventricle also affects the subvalvular apparatus of the mitral valve and may lead to valvular dysfunction (see Chapter 12).
Look at the shape of the ventricle! It provides important diagnostic clues! Slim ventricle Hypertrophy Spherical Dilated cardiomyopathy, reduced LVF, volume overload Apical ballooning Stress cardiomyopathy / Tako-Tsubo Spade-shaped Apical hypertrophic cardiomyopathy Distortion Myocardial infarctions/aneurysms/remodeling Banana-shaped Hypertrophic cardiomyopathy