
1. Introduction to Carotid Ultrasound


/* .lity-iframe-container iframe { background: #fff !important; } */ .articles__categories nav { display: none !important; } .sonopl-book__aside .articles__categories { background: #f5f5f5; } .sonopl-article th, .sonopl-article td { color: black; text-align: left; } function advagg_mod_1() { // Count how many times this function is called. advagg_mod_1.count = ++advagg_mod_1.count || 1; try { if (advagg_mod_1.count <= 40) { var getClass = document.querySelectorAll(".articles__categories"); var a = document.createElement('a'); var linkText = document.createTextNode("Get Carotid MC Free Lectures"); a.appendChild(linkText); a.title = "newsletter"; a.href = "/overlay/forms/cu_mc/16618"; a.setAttribute("class", "sonopl-button sonopl-button--default"); a.setAttribute("data-lity", ""); a.style = "line-height: 1.2;margin-top: 25px;padding: 15px;width: 100%;"; for(var ix = 0; ix < getClass.length; ix++) { getClass[ix].appendChild(a) } // Set this to 100 so that this function only runs once. advagg_mod_1.count = 100; } } catch(e) { if (advagg_mod_1.count >= 40) { // Throw the exception if this still fails after running 40 times. throw e; } else { // Try again in 250 ms. window.setTimeout(advagg_mod_1, 250); } } } function advagg_mod_1_check() { if (window.jQuery && window.Drupal && window.Drupal.settings) { advagg_mod_1(); } else { window.setTimeout(advagg_mod_1_check, 250); } } advagg_mod_1_check();
1.1 What is carotid (duplex) ultrasound?
Carotid ultrasound (also called carotid duplex sonography or scan) is one of the most important ultrasound imaging modalities in medicine. It allows us to assess cerebrovascular risk and diseases such as: carotid plaques, carotid artery obstruction (stenosis) and many other pathologies (i.e. dissection, aneurysms, fibromuscular dysplasia). The term “carotid ultrasound” is a bit misleading, since it is mandatory during the procedure to also scan the vertebral arteries. So actually the term “extracranial cerebrovascular Duplex sonography” would be more appropriate.
The carotid artery is “representative” of other arteries in the body (i.e. coronary arteries). This is why carotid ultrasound also allows us to assess the overall burden of atherosclerosis (and therefore the risk of cardio- cerebrovascular events). Carotid ultrasound provides high-resolution images that also allow us to study the intima media thickness, detect plaques and to grade stenosis.
Important treatment decisions are made based on carotid ultrasound such as:
- Should the patient be treated medically?
- Is a surgical procedure (endarterectomy) or stenting required?
- Can other surgical procedures (i.e cardiovascular surgery) be performed safely
Example of a normal carotid ultrasound scan:
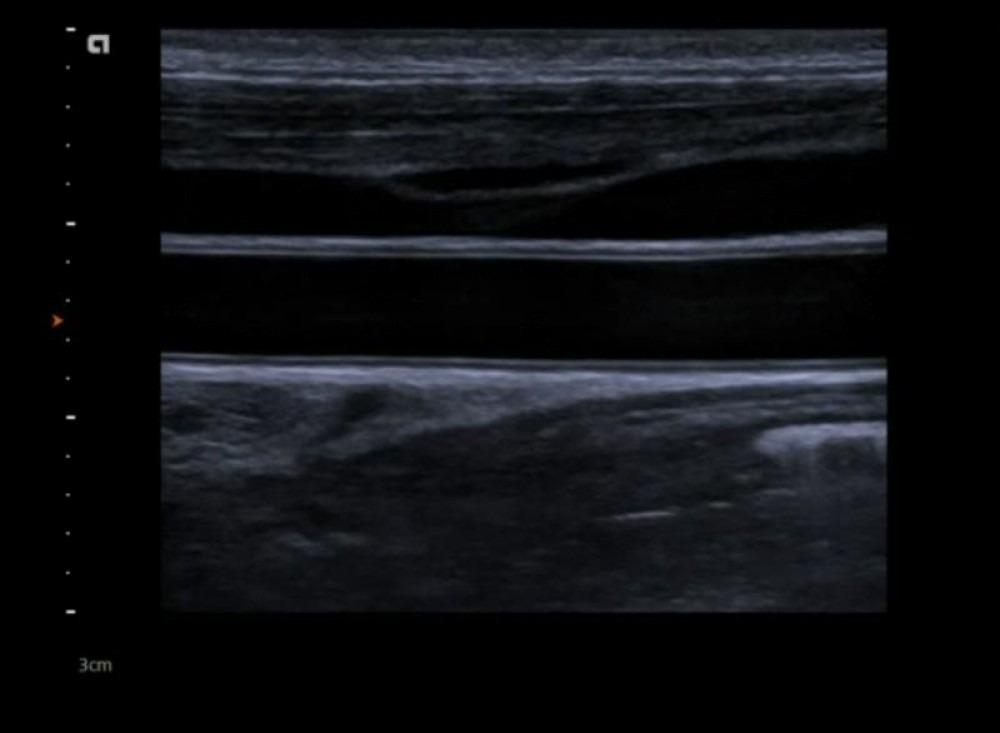 Normal carotid ultrasound (Duplex scan) of the common carotid artery. The arterial wall and its layers (intima media complex) is nicely depicted.
Normal carotid ultrasound (Duplex scan) of the common carotid artery. The arterial wall and its layers (intima media complex) is nicely depicted.
Example of a mixed plaque:
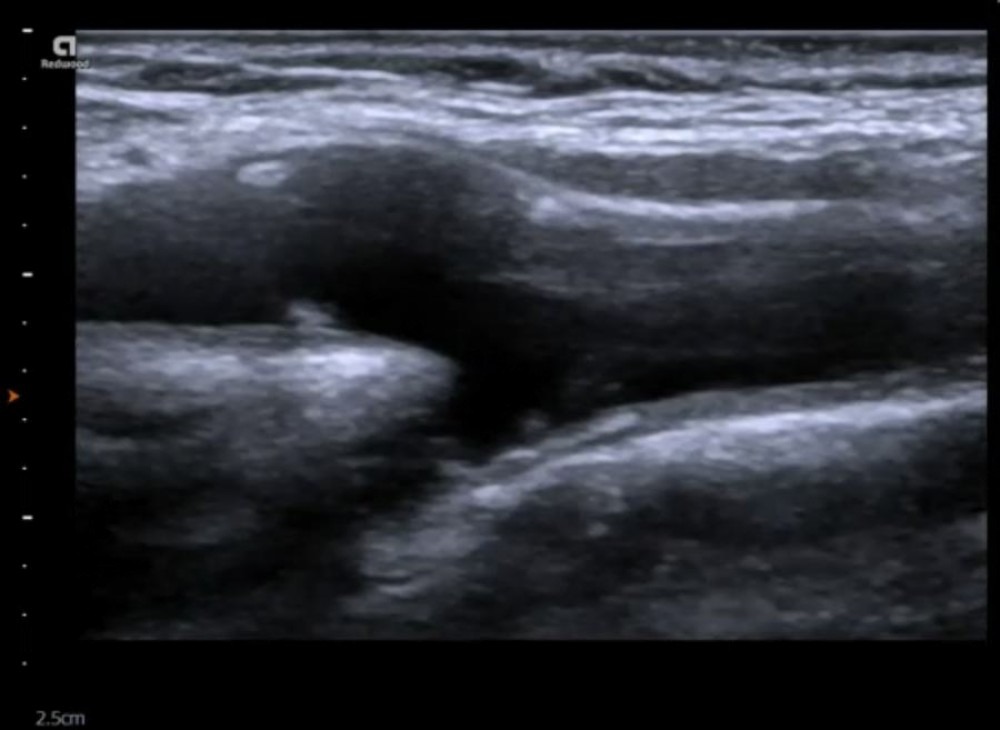 Carotid ultrasound (Duplex scan) of the bifurcation demonstrating small (haemodynamically insignificant), mixed plaque (partially calcified plaques)
Carotid ultrasound (Duplex scan) of the bifurcation demonstrating small (haemodynamically insignificant), mixed plaque (partially calcified plaques)
1.2 What are the indications of carotid duplex ultrasound?
- Evaluation of patients with hemispheric neurologic symptoms, including stroke, transient ischemic attack, and amaurosis fugax
- Evaluation of nonhemispheric or unexplained neurologic symptoms
- Evaluation of patients with a cervical bruit
- Evaluation of pulsatile neck masses
- Preoperative evaluation of patients scheduled for major cardiovascular surgical procedures
- Follow-up evaluation of patients with proven carotid disease
- Evaluation of postoperative post interventional (carotid endarterectomy, stenting, carotid-to subclavian artery bypass
- grafting)
- Intraoperative monitoring of vascular surgery
- Evaluation of patients with carotid reconstruction after extracorporeal membrane oxygenation bypass
- Screening of high risk patients; atherosclerosis elsewhere
- Evaluation of suspected subclavian steal syndrome
- Evaluation for suspected carotid artery dissection, arteriovenous fistula, or pseudoaneurysm
- Evaluation of patients with syncope, seizures, or dizziness
- History of head and neck radiation
1.3 What are the limitations of carotid duplex ultrasound?
- Vessels are small (0.3-1.5cm), good hand eye coordination required
- We only see the extracranial arteries
- The origin of the common carotid arteries difficult to image
- The vertebral arteries difficult to see DD hypoplasia or complete occlusion of the vertebral arteries
- Rely on indirect signs to quantify intracranial stenosis
- Sometimes difficult to differentiate the ECA from the ICA
- Calcifications make grading of stenosis difficult
- Trauma (cervical collar)
- Image quality
1.4 How to perform Carotid Duplex ultrasound?
Carotid (Duplex) sonography is performed either by sonographers (Registered Vascular Technologist- RVT) or medical doctors (internists, angiologists, cardiologists, radiologists, vascular surgeons). There is also an increased interest in carotid duplex sonography by family doctors, general practitioners and health care professionals working in a primary care setting.
- Carotid US is performed with a linear transducer, with a frequency between 7-12mHz.
- The linear transducer has the advantage that it has a large aperature (footprint) and that provides high-resolution images of structures which are superficial (such as the carotid artery)
- The patient is positioned on the back with the head turned to the contra-lateral side of the vessel, which is scanned
- The observer is positioned either at the head, to the left or to the right of the patient.
- Scanning can be performed with the left or right hand. Some also switch the scanning hand depending on which side / carotid artery is investigated.
- Both longitudinal and transverse planes are used for scanning
1. 5 What are the risks of carotid (duplex) ultrasound?
Ultrasound in general is a very safe and painless procedure. It does not generate any harmful radiation. Ultrasound does not cause any harm to the tissue and there is no risk that manipulation with the transducer dislodges a plaque and causes a stroke. It is equally unlikely that asystole or clinically significant bradycardia can be provoked during a scan (hypersensitive carotid sinus).
1.6 How to learn carotid (Duplex sonography) ultrasound?
Carotid ultrasound is not difficult to learn. It is probably easier to learn than some other ultrasound imaging modalities. It requires knowledge of:
- The physics of ultrasound
- Instrumentation and “knobology” (features and function of a scanner)
- Anatomy (vessels and other structures of the neck)
- Ultrasound anatomy
- Imaging skills (how to acquire high-quality images)
- Cerebrovascular pathologies (plaque, stenosis, dissection, fibromuscular dysplasia
- Practical skills – as all other US imaging modalities it is important to train your eye- hand coordination
If you are already practicing ultrasound (i.e. abdominal ultrasound or echocardiography) you already have a head start. Get a linear transducer and simply start imaging. There are numerous books, onsite and online seminars /courses that will help you to acquire the skills to learn carotid ultrasound. Ultrasound schools also teach vascular / carotid ultrasound. Most important though stay curious and use every opportunity you have to scan patients!
.pagination .pager .pager__item { font-size: 12px; } .pagination .pager .pager__item--current { padding: initial; } .pagination { margin: 0; margin: 0 auto; margin-top: 0 !important; } .pager { margin-top: 0 !important; padding: 0; display: flex; } .pagination .pager { padding: 0; } .pagination .pager a { padding: 8px 12px; } .pager__item a { box-shadow: none !important; } .aut-nav-carotid-p { text-align: center !important; margin-bottom: 6px !important; } function advagg_mod_2() { // Count how many times this function is called. advagg_mod_2.count = ++advagg_mod_2.count || 1; try { if (advagg_mod_2.count <= 40) { var autNaviCarotid1 = ('\ \- \
- \
Chapters\
\
- \ 1\ \
- \ 2\ \
- \ 3\ \
- \ 4\ \
- \ 5\ \
- \ 6\ \
- \ 7\ \
- \ 8\ \
- \ 9\ \
- \ 10\ \
- \ 11\ \
- \ 12\ \
- \ 13\ \
- \ 14\ \
- \ 15\ \
- \ last »\ \ \ \ '); var autNaviCarotid2 = ('\
Carotid Ultrasound Webbook & Wiki\ \
- \
- \
‹ previous\
\
- \ BACK TO OVERVIEW\ \
- \ next ›\ \ \ \ '); (function($) { $(document).ready(function(){ $(".sonopl-article.sonopl-book__content.sonopl-content-main") .prepend(autNaviCarotid1) .prepend(autNaviCarotid2); $(".aut-nav-carotid") .prepend(autNaviCarotid1) .prepend(autNaviCarotid2); }); }(jQuery)); // Set this to 100 so that this function only runs once. advagg_mod_2.count = 100; } } catch(e) { if (advagg_mod_2.count >= 40) { // Throw the exception if this still fails after running 40 times. throw e; } else { // Try again in 250 ms. window.setTimeout(advagg_mod_2, 250); } } } function advagg_mod_2_check() { if (window.jQuery && window.Drupal && window.Drupal.settings) { advagg_mod_2(); } else { window.setTimeout(advagg_mod_2_check, 250); } } advagg_mod_2_check();
If you like the way we teach, please leave a message!
- \ BACK TO OVERVIEW\ \
- \ 1\ \