
Writing an Ultrasound Report – Secrets: Part 3 Biggest Mistakes


Dear Colleague,
are you ready for the biggest mistakes that ultrasound specialist make when they write a medical report? I know most of us focus on the exam itself but what good are the best imaging and diagnostics skills if the results are not communicated appropriately.

1) The “anecdotal” ultrasound exam
No report is written at all - the findings are communicated verbally.
This practice is more common than you might think; Especially, if the ultrasound exam is performed on an intensive care unit, the emergency room or on the ward. Often it involves critically ill patients where proper documentation and reporting would really make a difference.
How much can you trust verbal descriptions of what someone saw? Would you base your medical decisions on such “anecdotal” results? Lack of time is often just an excuse not to write a report. In my experience it is more often insecurity, inexperience and fear of making a false statements that lead to this habit.
Here is my tip if you are uncertain: Store the images (as many as possible) and discuss them with someone who is more experienced. Write a preliminary report and don’t be afraid to make mistakes.
Discipline yourself to always write a complete exam. It will ultimately accelerate your learning curve.

2) The vague report
What do you do with the following statement?
 Example of a “vague” statement: Avoid words such as “appears” could, would, possible etc.
Example of a “vague” statement: Avoid words such as “appears” could, would, possible etc.
Yes, we all have our uncertainties, but vagueness neither helps the referring physician nor your career. There are times where you need to come to a decision. This does not mean that you cannot leave a “back door” open. Here is an example:
“Hyperechoic mass in the blabla (DD reverberation artifacts)”.
No matter if a tumor is present or not, with this phrasing you can never “loose”. But, you still point the referring physician to a potential pathology.
3) Over-description
I remember reading a report of a colleague where an entire page was dedicated to the description of the mitral valve: the echogenicity of each leaflet and segment, the presence of small calcifications, the degree of thickening, the motion of the valve practically every chord was mentioned in the report. While, the report was quite amusing it was literally “unreadable”. The relevant message did not stand out: Namely: that the patient had abnormalities related to a previous endocarditis. The bottom line: Make sure that the main message is clear and easy to understand.
My tip: Write a summary with potential next steps.
This brings me to a strategic mistake that is frequently made:
4) Patronizing the referring physician
You might be a super expert, and have a clear view how to manage the patient based on your findings. But when you write a report you need to find the fine line between helping the referral doctor and patronizing him. I know it is hard, but if you really want to help the patient, grab the phone and communicate directly with the physician. Gently guide him to the next steps and don’t take control of patient management (unless it is your patient). Physicians have different expectations from a report and patronage is a major reason why some will never refer a patient to you again.
And here is another killer mistake:
5) “Abbreviatitis”
Health care professionals rarely have time, but while saving a little bit of time by using abbreviations you steal time from those who try to decipher your report. Not all physicians are cryptologists. Take a look at the following text:
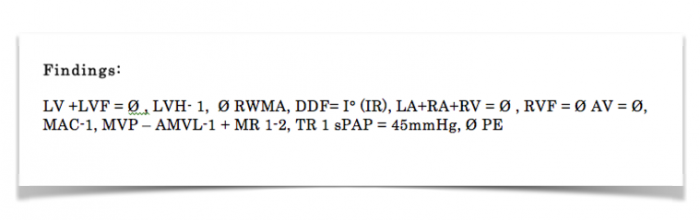 Example of a report that only consists to abbreviations.
Example of a report that only consists to abbreviations.
If you are not a cardiologist you might be familiar with the abbreviations but all others will ultimately fail to understand your report.
My tip is simple: don’t use any abbreviations at all!
6) Unanswered Questions
It is the same all over the globe: As ultrasound specialists we suffer from the poor quality of referrals. Why was the patient sent? What is the underlying problem in the first place? Why do we need to repeat the study, even though the patient had an ultrasound exam only a few days ago? Clearly, it is important to educate the referring physicians. But I often see reports where the question is left unanswered. One phrase is enough to signal to the referring physician that you actually read the referral question.
Here is a tip: Talk to the patient and take a glance at the patients chart and put yourself in the driving seat of the treating physician. This will help you to answer referral question even if they were never stated. For example, in a patient with valvular heart disease it will be important to mention if ventricular function deteriorates and if surgery is indicated. In a patient with cancer and chemotherapy it will be important to state if there is disease progression.
There is much you can do wrong when writing a report, but how do you write a really good report? You will find out shortly. In the next part of our series on reporting we will discuss how to structure your report and what should be included.
In the meantime I would be curious to know what your biggest pain is when it comes to writing a report
Best Thomas and the 123sonography team