
A Trip to China


Don’t we all think that our little workplace is the center of the universe? That our problems, patients, and the way we go about treating them is the only reality? If you read on you will find out that medicine is practiced differently in other parts of the world.
 Echo course at the Jilin Heart Hospital.
Echo course at the Jilin Heart Hospital.
The Jilin Heart Hospital - A medical oasis
Last April I had the opportunity to teach echocardiography in China - to be specific, in the north-eastern part of the country, in the city of Changchun (province of Jilin). You might have never heard of Changchun, but I bet it is probably larger than the town you come from. Changchun is the 10th largest city in China, yet the hometown of nearly 10 million people. The Jilin Heart Hospital at which I lectured is not representative of the health care system in China. In contrast to many other hospitals in the country, it is a modern building equipped with all types of high-end technologies.
 Jilin Heart Hospital.
Jilin Heart Hospital.
Thanks to Harry Huang and Roland Fasol the chief cardiovascular surgeon and his team, the hospital is now able to provide state-of-the-art services such as heart catheter and cardiovascular surgery to patients in this region. However, the Jilin Heart Hospital is mere drop in the ocean. Patients in China still die from conditions that could be easily treated, such as simple atrial septal defects, PDA´s, or mitral and aortic valve disease. Most of these conditions are not even diagnosed.
 Dr Liu Guangyo, Thomas Binder, Wenwen Du, Dr. Qi Xiuje.
Dr Liu Guangyo, Thomas Binder, Wenwen Du, Dr. Qi Xiuje.
 Harry Huang and Roland Fasol.
Harry Huang and Roland Fasol.
A glimpse at the problem
There is another disease that is on the rise in China: coronary artery disease. The Chinese are getting accustomed to an unhealthy lifestyle. More than 50% of the population smoke and hypertension often goes by untreated. Today I want to show you a patient whom I investigated while I was in Changchun. A case with a unique finding. Read on to find out more.
Puffing early
Yu, a policeman, had been smoking for 20 years and had a history of coronary artery disease. He was brought to the hospital at the age of 58 with dyspnea.His echo clearly shows why he has dyspnea. His left ventricular function is poor and he also has regional wall motion abnormalities. Let us take a closer look at these.
 Four-chamber view showing reduced left ventricular function.
Four-chamber view showing reduced left ventricular function.
Note that the mid- and basal inferior septum is dyskinetic and the myocardium is rather echogenic. This is definitely a scar. But which coronary vessel is involved? To fully understand the condition we need to look at the other views:
 Two-chamber view: inferior akinesia.
Two-chamber view: inferior akinesia.
The scar extends to the inferior wall (basal and mid). While rotating further counterclockwise, we saw a scar in the posterolateral region.
 Apical long-axis view. The scar is also seen posterolaterally.
Apical long-axis view. The scar is also seen posterolaterally.
Does the scar extend even further? Into the lateral region? To answer this I recommend you rotate further or start out from a four-chamber view and rotate clockwise until you see this view:
 Lateral view of the myocardium.
Lateral view of the myocardium.
This view might look like a five-chamber view, but it is not one. It shows you more of the lateral wall. We also see a wall motion abnormality here.
Which vessel?
I would say he has a pretty big infarct, right? Coronary angiography showed a huge proximately occluded right coronary artery. Does echo allow us to clearly say which vessel is involved? I would say not always, but most of the time. Here is a little trick: if the inferior septum is involved it HAS to be the right coronary artery. Sure, the circumflex artery may also be involved.
How does the information help?
First we established the diagnosis (CAD). We know why he has dyspnea. It showed us that the patient is very unlikely to benefit from revascularization of the right coronary artery. After all, the myocardium is already scarred and dead.
A second look
While you were looking at the regional wall motion: did you note another peculiar aspect of the echo? I will show you what I mean:
 Tear in the interventricular septum.
Tear in the interventricular septum.
There is a tear at the rim of the scar right in the interventricular septum. This is actually a typical site of ischemic VSD's.
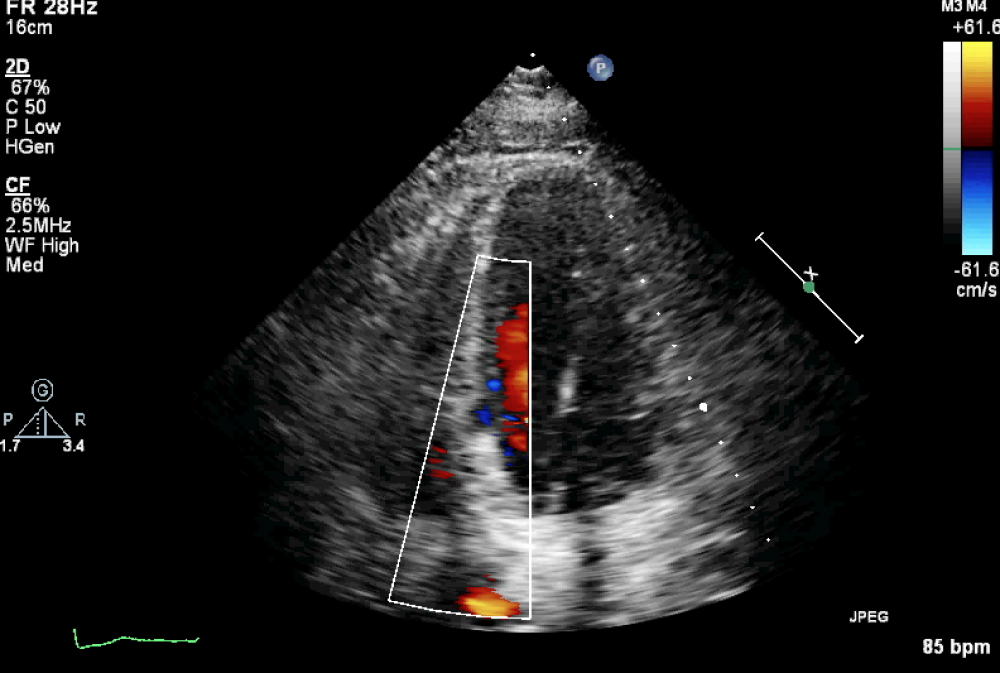 Flow can be seen within the fissure, but no VSD flow is present.
Flow can be seen within the fissure, but no VSD flow is present.
One can even see blood flow into the tear. Fortunately, there is no shunt flow across the septum so this may also be termed an “incomplete” septal rupture. Yu was lucky in that complete rupture did not occur at the time of the infarct. Now that a scar has formed, the tissue is too firm to rupture completely. So I don't think Yu has any reason to worry.
Imagine picking up such a finding in the early phase of an infarct! Wouldn’t this change your approach to the patient? I bet you would monitor him very closely with the scalpel in your hand.
A few tips
- If you want to detect such small findings that can make a difference for your patients, consider joining our Masterclass.
- If you are interested in seeing how people in other parts of the world use echocardiography, check out these newsletters:
The African "Beauty" and its "Beast"
North “Stars” and Aortic Stenosis
Best,
Thomas
PS: Don’t forget to “like” our Facebook page. More teaching material is awaiting you there.
Related Courses

The Echo MasterClass is a premium online training program that will bring your echo skills to…
The Echo BachelorClass provides an invaluable foundation for the practice of echocardiography…