
Gemini Part II



Remember in the article "Gemini I" I promised to report on the outcome of the pregnant woman who developed heart failure and mitral regurgitation? Well, here is the sequel. It was a very difficult decision. As many of you suggested, we did not want to put Brigitte’s life at risk. Her pulmonary pressure was more than 70 mmHg. Shortly after we recorded the images, a cesarean section was performed. All went well and both twins are fine. They do need special attention, but are currently stable.
What about Brigitte?
She was also fine after the cesarean section. Her dyspnea had resolved and she was smiling. Obviously, the thing that interested us next was the severity of her mitral regurgitation. Just as a reminder - here is a video clip showing her mitral regurgitation before the cesarean section:
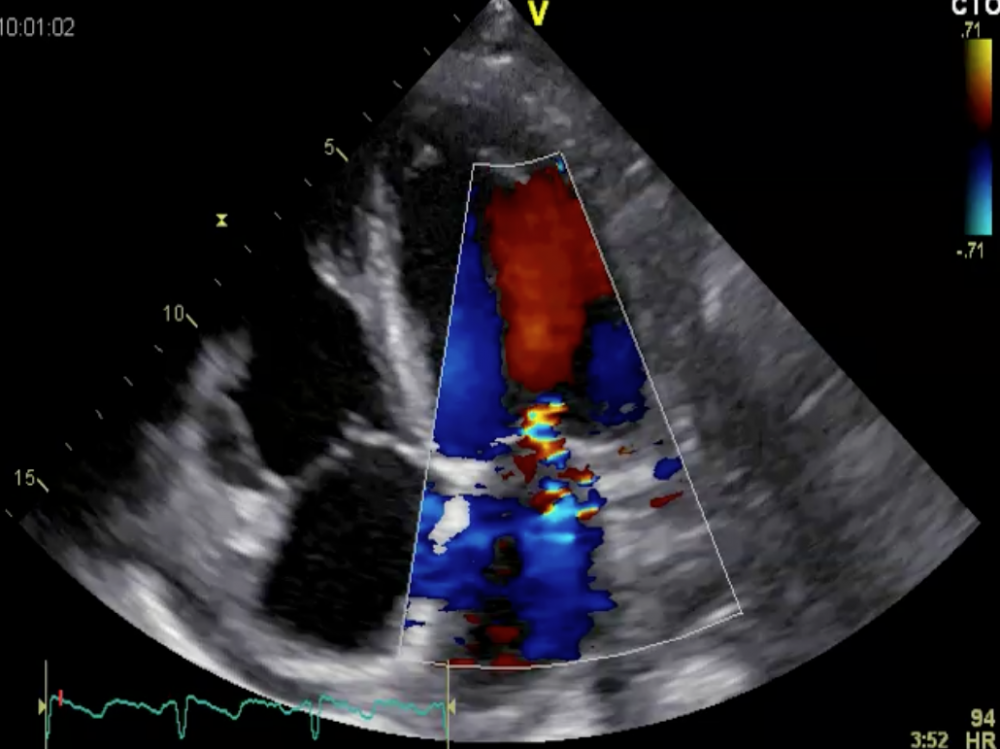 Mitral regurgitation in a pregnant woman (25 weeks of gestation)
Mitral regurgitation in a pregnant woman (25 weeks of gestation)
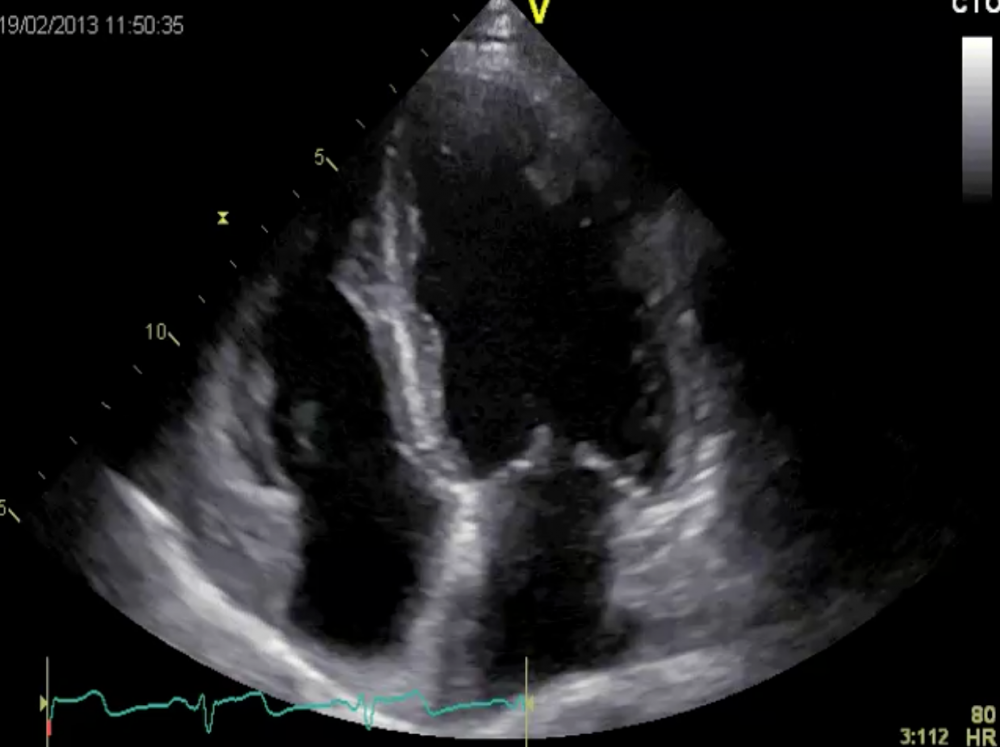
We rated her regurgitation moderate to severe. How severe is it now – just a few days after the cesarean section? Here is the four-chamber view:
 Four-chamber view after pregnancy
Four-chamber view after pregnancy
As expected, her mitral regurgitation had abated significantly. It was mild. No wonder she is doing better now. Our hypothesis that the cause of mitral regurgitation was functional proved true. Her intravascular volume is less than it was during pregnancy, and her blood pressure dropped. This contributed to the reduction of mitral regurgitation.
The ventricles next to each other
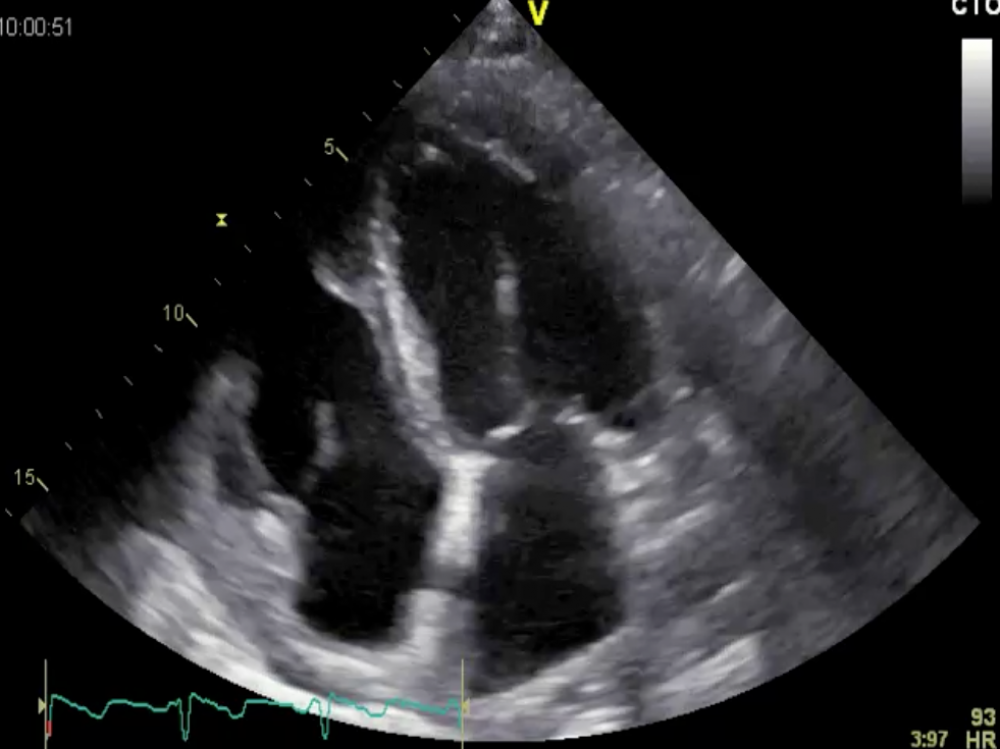
Now we will take a closer look at left ventricular function:
 Four-chamber view. How would you grade left ventricular function?
Four-chamber view. How would you grade left ventricular function?
Ejection fraction is normal at 67%. End-diastolic volume was 111 ml. Just for comparison - this is what the left ventricle looked like during pregnancy:
 Four-chamber view during pregnancy
Four-chamber view during pregnancy
At the time, end-diastolic volume was 123 ml and ejection fraction 69%. On comparison, the left ventricle is slightly smaller and its function pretty much the same after pregnancy. But these figures are somewhat misleading. As regurgitation causes volume overload, one would expect ejection fraction to be higher under these conditions.
Is myocardial function truly normal?
Despite the patient’s apparently normal ejection fraction, one must ask oneself whether her contractility is truly normal. I have my doubts. Look at the short-axis view of the ventricle:
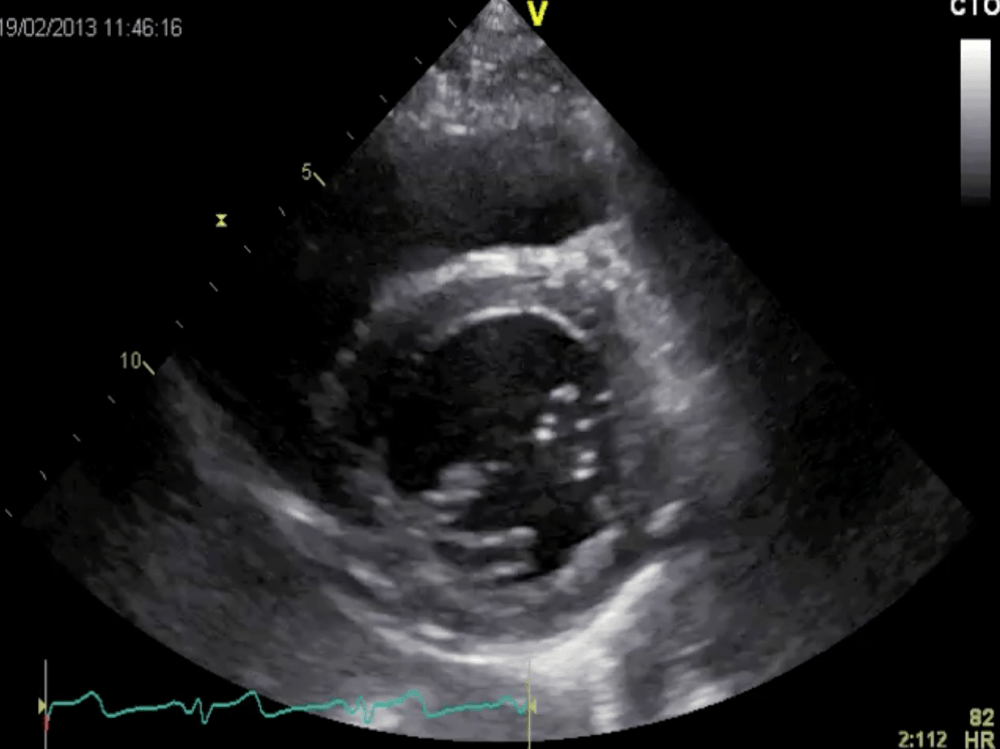 Short-axis view after pregnancy
Short-axis view after pregnancy
I would say her radial function is reduced. What about longitudinal function? We repeated speckle-tracking analysis, performed apical views, and obtained the following:
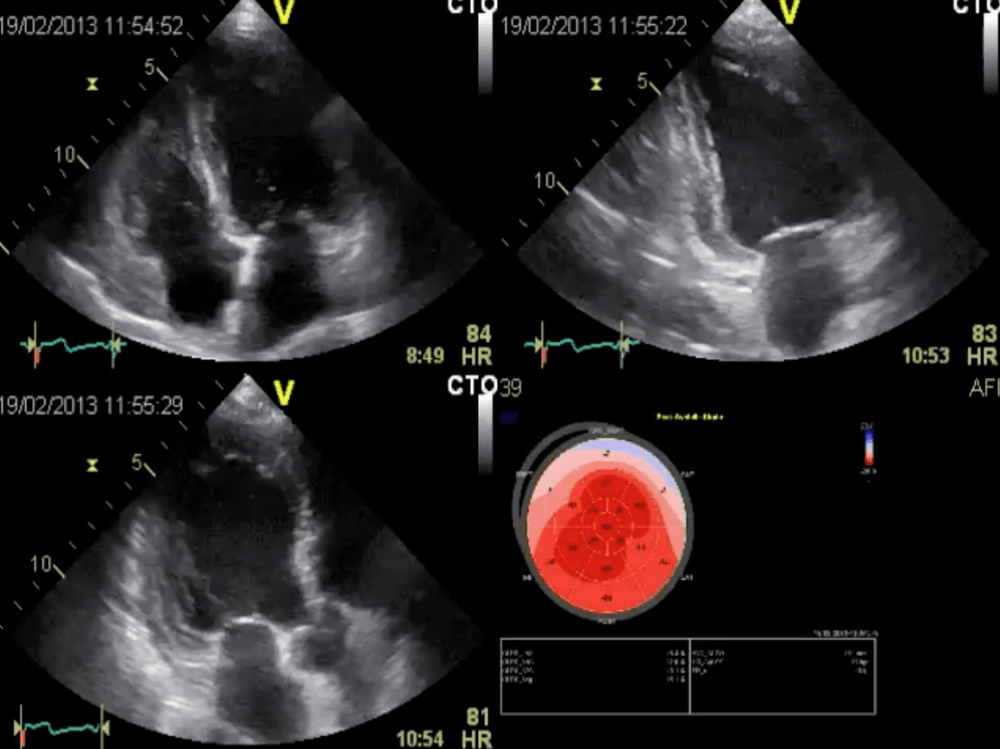 Apical views and speckle tracking analysis (bull’s eye) of longitudinal function. Again, we find an abnormal strain pattern.
Apical views and speckle tracking analysis (bull’s eye) of longitudinal function. Again, we find an abnormal strain pattern.
The pattern is similar to the previous study. Apical segments are hypercontractile while longitudinal function is reduced in the basal segments.
Summing up
I would interpret the findings as follows: Brigitte had functional mitral regurgitation during pregnancy. I am not sure why. Patients with preeclampsia usually have a reduced intravascular volume. Maybe the fact that she had a twin pregnancy and hypertension was a contributing factor. Still, I believe that severe functional mitral regurgitation can only occur in the presence of at least some degree of left ventricular dysfunction. I am convinced her myocardial function is not completely normal despite her normal ejection fraction. She has type I diabetes and was under insulin. This predisposes an individual to diseases of small vessels and coronary arteries. Besides, these conditions are known to be more common in patients with preeclampsia.
I told Brigitte to return for a second look after she had recovered fully. When she returns, we will perform additional tests to rule out coronary artery disease.
Related Courses

This course aims to provide you with the knowledge and skills on how to do an ultrasound…

Neonatal and Pediatric Ultrasound BachelorClass covers a wide range of POCUS applications in…
The OB/GYN Ultrasound BachelorClass is a clinical course that will provide you with in-depth…