
From Gluten Intolerance to Oncology: When Mesenteric Lymphadenopathy Tells a Bigger Story

Presented by Andrei Satsuk, MD at the Scientific and Practical Conference “Modern Aspects of Neurological Diagnostics and Pediatric Ultrasound”, St. Petersburg, May 16, 2025
Case Summary
A 12-year-old boy with biopsy-confirmed celiac disease, diagnosed in 2023, was referred for ultrasound evaluation because of persistent fatigue, chronic anemia, and recurrent abdominal pain.
Despite strict adherence to a gluten-free diet, his weight continued to decrease, and laboratory tests revealed elevated inflammatory markers (CRP 140–200 mg/L, ESR 50–70 mm/h) and low hemoglobin (~85 g/L).
The patient had a known history of splenomegaly since early childhood, previously attributed to recurrent infections. He also suffered from chronic iron deficiency anemia requiring repeated transfusions, though his iron profile was atypical-low serum iron but normal or elevated ferritin, suggesting anemia of chronic inflammation.
Albumin and total protein were decreased, consistent with malabsorption, while LDH, AFP, and liver function tests were normal.
Ultrasound Findings
Comprehensive abdominal and retroperitoneal ultrasound was performed.
The liver, pancreas, kidneys, and biliary system showed no structural abnormalities.
The spleen, however, was markedly enlarged – length 130 mm, thickness 68 mm, confirming splenomegaly.
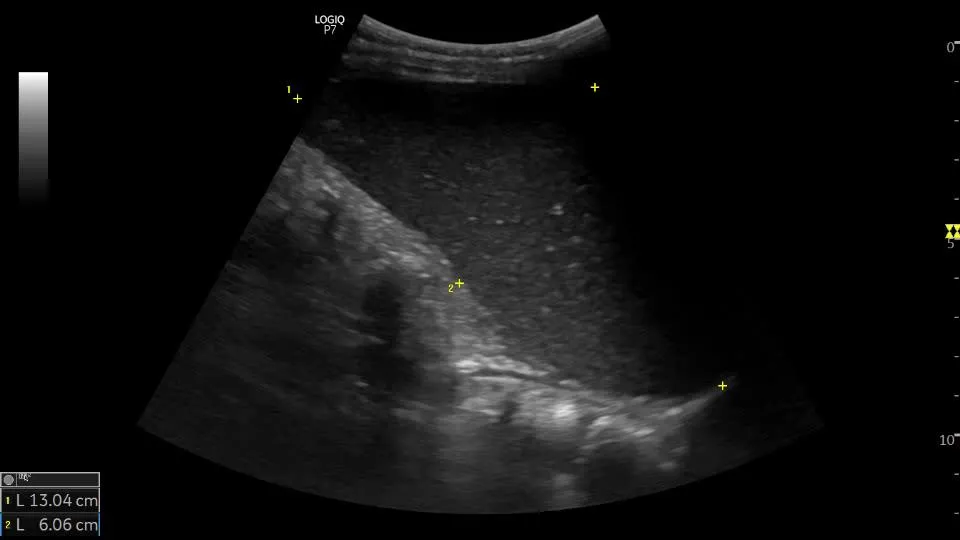
The key finding, however, was that of a mass in the mesogastric region. Have a look at the following loops and answer our quiz question!
Did you answer the quiz question in our video? If not, go back and watch now! Then continue to read the explanation!
Explanation:
Size: 44 × 35 × 39 mm
Shape: round
Contours: mostly well-defined margins, capsule shows focal discontinuity at the upper pole with peripheral infiltration
Internal structure: hypoechoic, no preserved layer differentiation, fine reticular echotexture
Vascularity: multiple feeding pedicles, mixed blood flow pattern
Adjacent tissues show signs of inflammatory or infiltrative changes
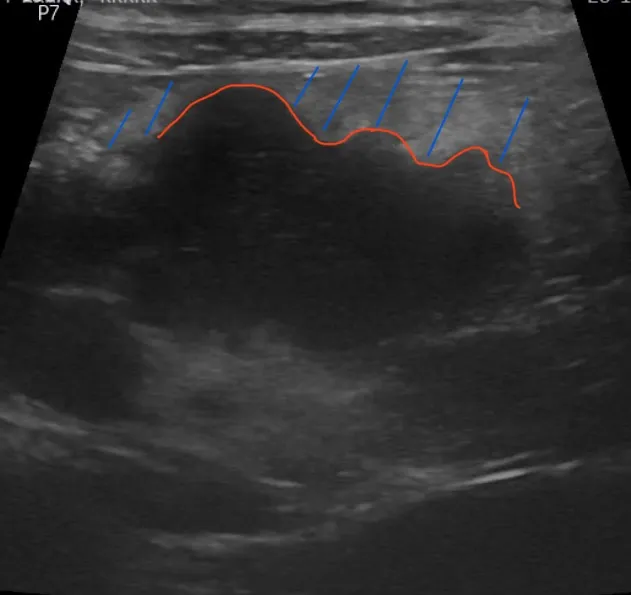
Additionally, there were at least 15 altered mesenteric lymph nodes clustered in the same region. They were found in the control study:
Size: Multiple nodules measuring 9 – 27 mm in diameter
Structure: heterogeneous, loss of normal corticomedullary differentiation
Contours: irregular, some forming conglomerates
Adjacent: The paranodal fat is infiltrated
When compared with a previous study from December 2024, the primary mass remained stable in size. However, newly altered mesenteric lymph nodes appeared, and splenomegaly had progressed — a worrisome evolution suggesting a systemic or proliferative process rather than a transient reactive change.
PET/CT Findings
PET/CT confirmed a metabolically active lesion in the left mesentery:
SUVmax 5.4, density 43 HU, size 4.7 × 3.7 × 4.4 cm
Additional lymph nodes with FDG uptake:
Mesenteric group: up to 1.6 cm (SUVmax 4.0)
Para-aortic group: up to 0.8 cm (SUVmax 1.6)
Aortocaval group: 0.6 cm (SUVmax 1.1)
No other metabolically active foci were detected.
Conclusion: Metabolically active mesenteric lesion and lymphadenopathy — findings most compatible with a lymphoproliferative process; morphological verification recommended.
Histopathological Findings
Biopsy material consisted of small fragments of lymphoid tissue with preserved architecture.
The lymphoid infiltrate was formed by secondary follicles with active germinal centers containing tingible-body macrophages and parafollicular zones rich in lymphocytes, plasma cells, and histiocytes.
Immunohistochemistry:
CD20: positive in follicular B-cells
CD23: positive follicular dendritic cell networks
CD30: scattered positive activated lymphocytes
CD58: expressed in histiocytic/macrophage populations
Ki-67: up to 80% in germinal centers, 5% in interfollicular zones
Interpretation: Reactive follicular hyperplasia of lymphoid tissue.
No definitive evidence of malignancy was found at that stage.
Differential Diagnostic Considerations
Given the clinical background of celiac disease, the main concern was the potential diagnosis of an enteropathy-associated T-cell lymphoma (EATL) — a rare, aggressive lymphoma arising in the setting of gluten-sensitive enteropathy.
Alternative diagnoses included:
- Infectious lymphadenitis (e.g., tuberculosis or yersiniosis)
- Castleman disease — a nonclonal lymphoproliferative disorder mimicking lymphoma both clinically and radiologically
Although histology favored a reactive process, the imaging evolution — stable primary mass with new abnormal nodes and increasing splenomegaly — raised suspicion for a slowly developing lymphoproliferative disorder.
Clinical Reflection
This case highlights the diagnostic challenge of differentiating reactive vs. neoplastic mesenteric lymphadenopathy in children, especially in the context of autoimmune enteropathy.
While initial histology showed no malignancy, dynamic imaging and clinical correlation revealed progressive systemic changes that could not be ignored.
For the sonographer and clinician alike, the lesson is clear:
“Abdominal ultrasound is not only about the liver, gallbladder, pancreas and spleen.”
Focused evaluation of hollow organs and mesenteric lymph nodes is essential, particularly in pediatric patients with chronic inflammatory or autoimmune conditions.
Ultrasound may be the first tool to reveal the systemic nature of the process — even when morphology still appears “benign.”
Take-Home Messages
Celiac disease can be associated not only with malabsorption but also with rare lymphoproliferative complications, such as EATL or Castleman disease.
Stable or enlarging mesenteric masses and progressive lymphadenopathy require close follow-up, even in the presence of reactive histology.
Comprehensive ultrasound assessment — including lymph node morphology, vascularity, and perinodal tissue — is crucial for early detection of atypical progression.
Interdisciplinary collaboration between radiology, gastroenterology, hematology, and pathology is key for accurate diagnosis and timely management.
Summary
A child with celiac disease, persistent anemia, and systemic inflammation developed progressive mesenteric lymphadenopathy and splenomegaly. Imaging findings suggested a lymphoproliferative process, while histology remained reactive. The case underlines the importance of dynamic imaging in detecting early malignant transformation and the vigilance required in chronic autoimmune diseases.
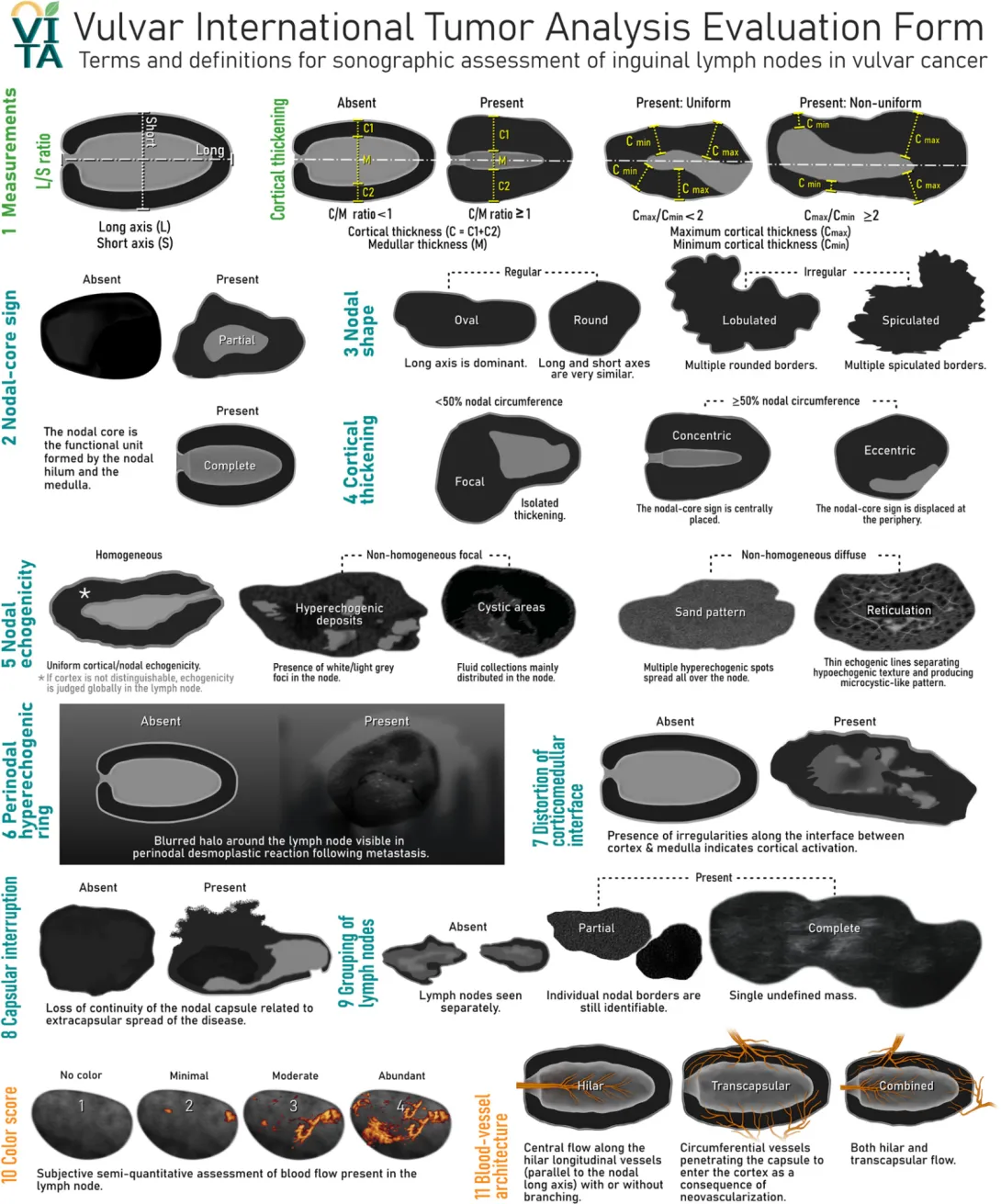
Structured assessment of lymph nodes.
Although there is currently no standardized or validated scoring system for the sonographic evaluation of intra-abdominal lymph nodes, the Vulvar International Tumor Analysis (VITA) evaluation form provides one of the most comprehensive and detailed frameworks for lymph node characterization. Originally developed for the assessment of inguinal lymph nodes in vulvar cancer, the VITA form systematically describes nodal morphology, cortical configuration, echogenicity, vascularity, and perinodal changes.
In the present case, a VITA-inspired descriptive approach was applied to intra-abdominal lymph nodes to ensure consistency and completeness of assessment. While some features (e.g., cortical thickness or perinodal halo) may not be fully visualized in deep abdominal locations, the conceptual structure of VITA – covering size and shape, internal architecture, echogenicity, vascular pattern, and surrounding tissue reaction – can be adapted to facilitate a standardized and reproducible report.
References
Lymph node characterisation and reporting:
- Fischerova, D., Garganese, G., Reina, H., Fragomeni, S.M., Cibula, D., Nanka, O., Rettenbacher, T., Testa, A.C., Epstein, E., Guiggi, I., Frühauf, F., Manegold, G., Scambia, G. and Valentin, L. (2021), Terms, definitions and measurements to describe sonographic features of lymph nodes: consensus opinion from the Vulvar International Tumor Analysis (VITA) group. Ultrasound Obstet Gynecol, 57: 861-879. https://doi.org/10.1002/uog.23617
- Chudobiński C, Świderski B, Antoniuk I, Kurek J. Enhancements in Radiological Detection of Metastatic Lymph Nodes Utilizing AI-Assisted Ultrasound Imaging Data and the Lymph Node Reporting and Data System Scale. Cancers. 2024; 16(8):1564. https://doi.org/10.3390/cancers16081564
Cases for comparison:
- McBride, Olivia M. B., Skipworth, Richard J. E., Leitch, Derek, Yalamarthi, Satheesh, Cavitating Mesenteric Lymph Node Syndrome in Association with Coeliac Disease and Enteropathy Associated T-Cell Lymphoma: A Case Report and Review of the Literature, Case Reports in Medicine, 2010, 478269, 4 pages, 2010. https://doi.org/10.1155/2010/478269
- Wu, Pao-Shu. “Mesenteric Castleman's disease: report of a case and literature review.” International journal of clinical and experimental pathology vol. 13,9 2397-2400. 1 Sep. 2020.
https://pmc.ncbi.nlm.nih.gov/articles/PMC7539862/ - Amy H. Pun, Harry Kasmeridis, Nicholas Rieger, Arun Loganathan, Enteropathy associated T-cell lymphoma presenting with multiple episodes of small bowel haemorrhage and perforation, Journal of Surgical Case Reports, Volume 2014, Issue 3, March 2014, rju013, https://doi.org/10.1093/jscr/rju013
- Ashjaei, Bahar et al. “Abdominal Mass Caused Failure to Thrive in a Young Boy: Mixed-Type Localized Retroperitoneal Castleman Disease.” Case reports in oncology vol. 13,2 853-856. 16 Jul. 2020, doi:10.1159/000508531
Related Courses

The Abdominal Ultrasound BachelorClass introduces you to one of the most important ultrasound…

Neonatal and Pediatric Ultrasound BachelorClass covers a wide range of POCUS applications in…

Learn about the origins of Pediatric Ultrasound, the relevant physics, selection of the right…