
Tour de France and the Heart – Part 2


How fast can you ride a bike? Can you reach a speed of 44 km/h? And I do not mean downhill. If you can, that's great. Can you also do it for 180 kilometers after you have swum a distance of 3.8 kilometers?
Introducing Georg
This is what Georg Swoboda is capable of doing. He is the Austrian triathlon champion and a successful competitor in many national and international Ironman events. His strength is cycling and there is only one triathlete in the world who was able to beat his cycling time of 4:07:43 over a distance of 180 km.
 Georg “Shurli” Swoboda; (http://www.georgswoboda.at)
Georg “Shurli” Swoboda; (http://www.georgswoboda.at)
To accomplish this you definitely need an extremely effective pump. In the first part of our Tour de France case stories we talked about the adaptations that occur in athletes (Tour de France - Part 1). Let us now take a closer look and discuss the echocardiographic findings in Georg. Similar to the cyclists on the tour, his heart should show adaptations related to what is known as “combined endurance and strength exercise”.
Super-effective pump
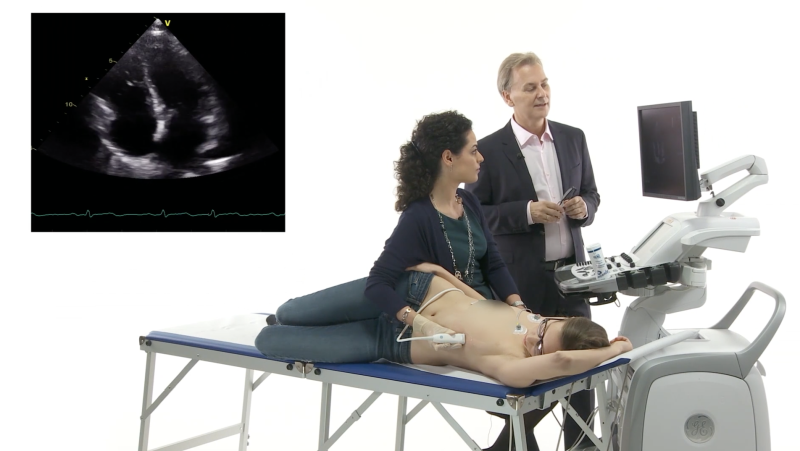
First we will take a look at the size of the heart. The end-diastolic diameter is 62 mm. Larger than normal indeed. Were you expecting a larger diameter? The truth is that, compared to untrained persons, the diameter of athletes' hearts is just slightly increased. The greatest increase is seen in those athletes (like Georg) who participate in combined endurance and strength sports. Left ventricular dilatation is more subtle after all other forms of training. But remember, even small changes in diameter can result in a significant increase in volume. This is simple geometry.
 Dilated left ventricle, with a low normal ejection fraction of 55%
Dilated left ventricle, with a low normal ejection fraction of 55%
Georg's left ventricle is not only wider but also longer; its length is 10.2 cm. So the end-diastolic total volume is 180 ml. This means that it can accommodate twice the amount of blood compared to a normal individual. His left ventricular function is low normal. We determined an ejection fraction of 55%. Does he have left ventricular dysfunction? No. His heart just works so effectively at rest that it does not have to contract more vigorously. With such a large ventricle, even low ejection fractions can generate high stroke volumes.
The right ventricle is important
In addition to the left ventricle, the right ventricle is also enlarged. This is a very frequent finding in athletes. Right ventricular function is definitely normal.
 Focusing on the right ventricle, which is dilated and shows hyperdynamic function
Focusing on the right ventricle, which is dilated and shows hyperdynamic function
As a matter of fact, his TAPSE (23 mm) is supernormal.
 TASPSE of 23 mm: this is a value you would rarely see in an untrained person at rest.
TASPSE of 23 mm: this is a value you would rarely see in an untrained person at rest.
This is an important finding because there has been some concern about prolonged exercise being harmful to the right ventricle. Transient RV dysfunction has been observed in this setting.
Left ventricular hypertrophy
We all know that athletes develop hypertrophy and that it can be difficult to distinguish this training effect from pathologic forms, such as those related to hypertension or hypertrophic cardiomyopathy. However, his septum measures 12-13 mm and shows just mild hypertrophy.
 M-mode, the septal thickness is 12-13 mm
M-mode, the septal thickness is 12-13 mm
In absolute terms this is not much. However, as the heart is enlarged it still amounts to a significant increase in myocardial mass (we established 186 g). Even in athletes who perform strength training you would rarely find a wall thickness exceeding 15 mm.
The Tiger in the Tank
What happens to the heart of an athlete when it has to perform at incredible levels? For instance, when the cyclists on the Tour are struggling up the Col du Tourmalet a "hors catégorie" and have to climb a distance of 17 kilometers at a gradient of 7.5%?
 Tour de France, Col du Tourmalet; John Kershner / Shutterstock.com
Tour de France, Col du Tourmalet; John Kershner / Shutterstock.com
The maximal oxygen uptake (VO2max) reflects aerobic physical fitness. It can be extremely high in athletes. For example, Lance Armstrong has a VO2max of 85 ml/kg/min, which is more than twice as much as that of an average young healthy individual.
Many adaptive processes occur in training. To find out how the heart contributes to these processes, we put Georg on a bicycle and performed a stress echo exam.
A walk in the park
At 350 watts of exercise, Georg was still comfortably talking to me. After all his aerobic – anaerobic threshold is somewhere close to 390 watts. During a normal competition he would cycle at 350 Watt this level for hours.
Georg unleashed
Look at his left ventricular function now:
 Four-chamber view during exercise
Four-chamber view during exercise
The size of the left ventricle is slightly increased. The ejection fraction of the ventricle is now 78% and his heart rate increased. All this taken together increases his cardiac output almost 5-fold during exercise.

How does the heart increase its ejection fraction? To look further we need to perform a speckle tracking analysis. Dr. Demanez explained how this new technology can help us to distinguish athletes' hearts from diseased hearts (Tour de France - Part 1). Now we will use this technique to better understand adaption to exercise:
The power of deformation
This is a comparison of longitudinal contraction between rest and exercise:

 Longitudinal strain at rest and during exercise
Longitudinal strain at rest and during exercise
Longitudinal function is normal at rest and increases significantly during exercise. So Georg's ventricle becomes shorter.
What is really interesting is that especially the inner layers of the myocardium are responsible for the increase in longitudinal function.
 Prominent longitudinal function of the subendocardial myocardial layer
Prominent longitudinal function of the subendocardial myocardial layer
Further analysis of Georg's heart during strain showed that all other deformation parameters, including radial and circumferential strain and strain rate, increased.
 Increase in circumferential strain during exercise
Increase in circumferential strain during exercise
What we learned:
In summary, athletes' hearts show numerous adaptations, both at rest and during exercise. Echocardiography helps us to understand much better why such a small pump is able to sustain such enormous workloads as those required when participating in events such as the Tour de France.
So the next time you watch the tour or any other sports competition, remember that it is also a kind of “a race of hearts”. Only those hearts that are best trained make it to the top. With an increasing number of individuals performing extreme sports, we physicians need to correctly interpret findings in athletes' hearts which, at first sight, can look quite similar to those of diseased hearts.
Best,
Thomas Binder

PS: Many thanks to Georg Swoboda and good luck for all further competitions

Related Courses
The Echo BachelorClass provides an invaluable foundation for the practice of echocardiography…