
How can I be sure that LVF is truly normal?
I am sure you have encountered the following problem: A patient comes with arrhythmias, to rule out myocarditis or because of dyspnea. Image quality is not the best and left ventricular function just doesn’t seem normal. Your calculations of ejection fraction are all over the place and you simply don’t trust them.
So, does the patient truly have cardiomyopathy or can you tell the patient everything is okay?
To master this situation here are five practical tips:
Tip 1: Rule out other abnormalities
Rule out other abnormalities such as left ventricular hypertrophy, valvular pathologies, dyssynchrony or regional wall motion abnormalities. The presence of other findings will increase the likelihood for LV dysfunction.
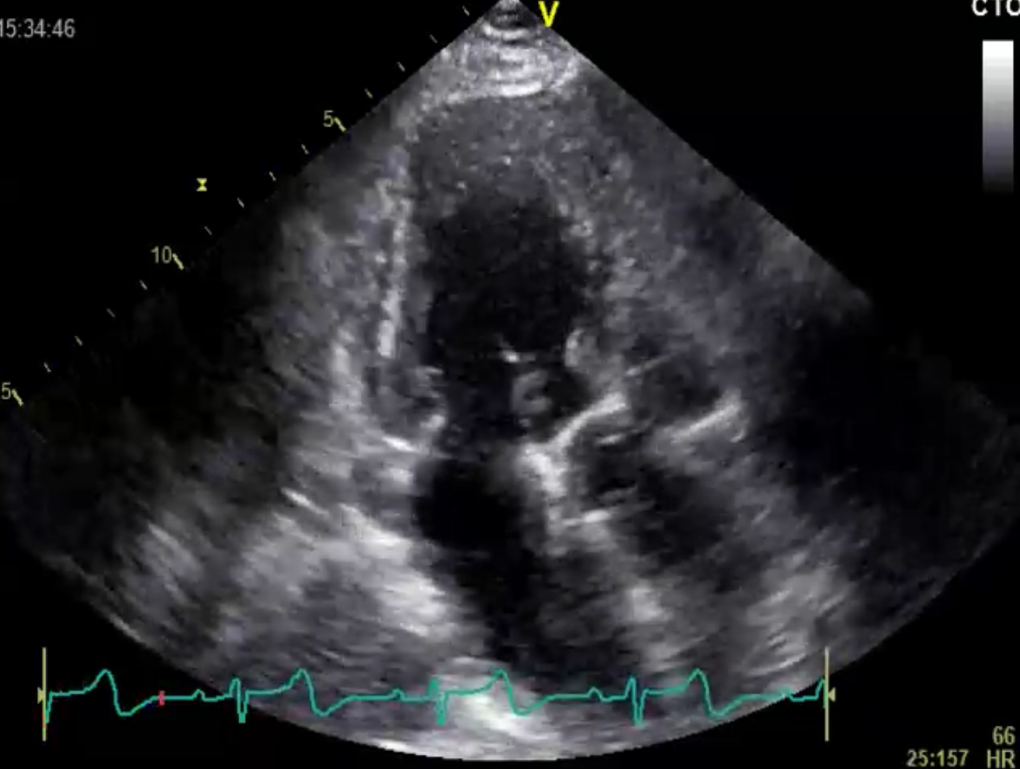
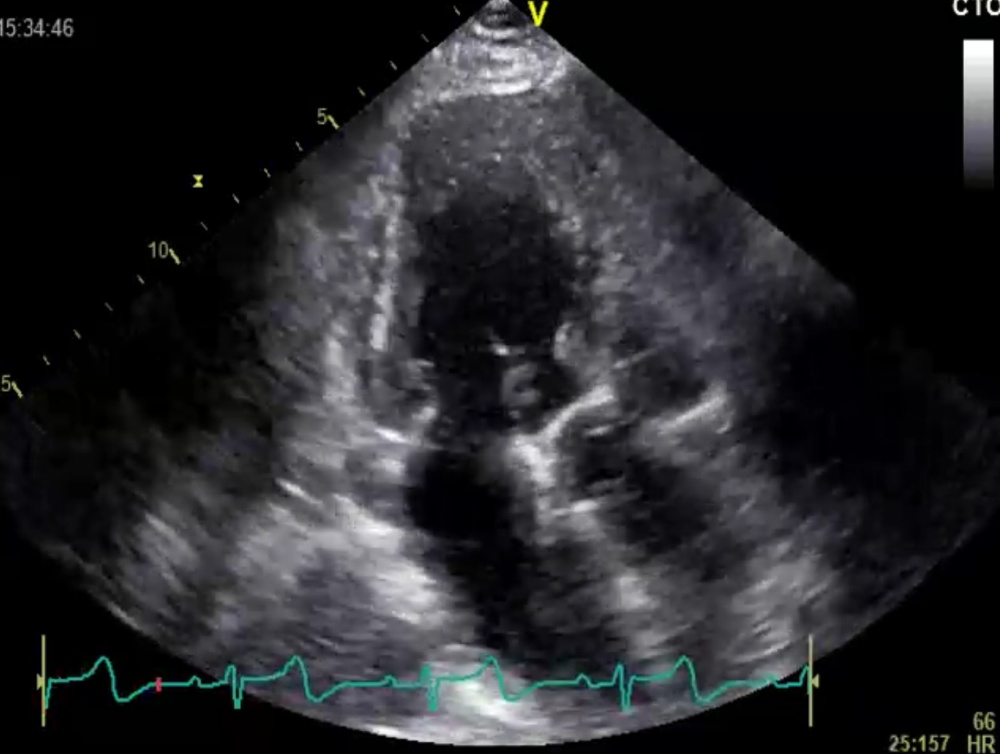 Example of a patient with left ventricular hypertrophy and mildly reduced LVF
Example of a patient with left ventricular hypertrophy and mildly reduced LVF
Tip 2: Try contrast
Try contrast! You will be surprised how much easier it is to quantify LVF if you can really see the endocardial boarders.
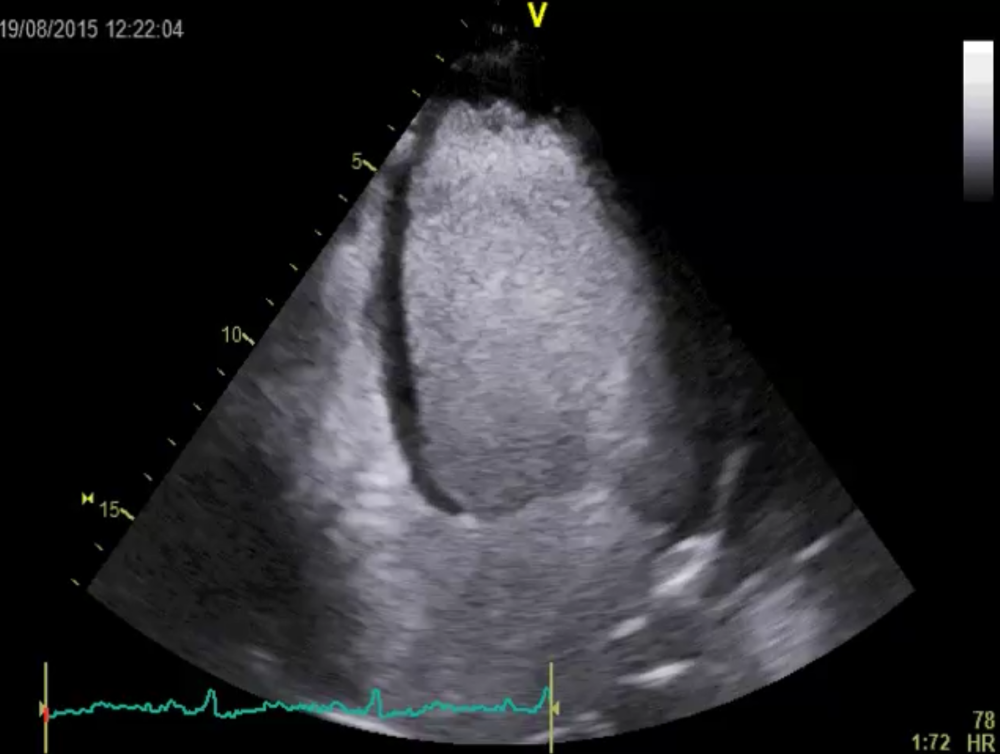 By using left ventricular contrast it becomes apparent that LVF is reduced
By using left ventricular contrast it becomes apparent that LVF is reduced
Tip 3: Focus on the motion of the mitral annulus
Focus on the motion of the mitral annulus. Get a feeling for the longitudinal function of the ventricle. Longitudinal contraction is a more sensitive parameter of function than radial function. You can even measure the mitral annular plane systolic excursion (MAPSE).
Tip 4: Use speckle tracking echocardiography (strain)
,,Use speckle tracking echocardiography (strain). If you find that peak global longitudinal strain is normal (>-18%) you practically excluded a cardiomyopathy. But be aware that athletes can also have “subnormal” longitudinal function.
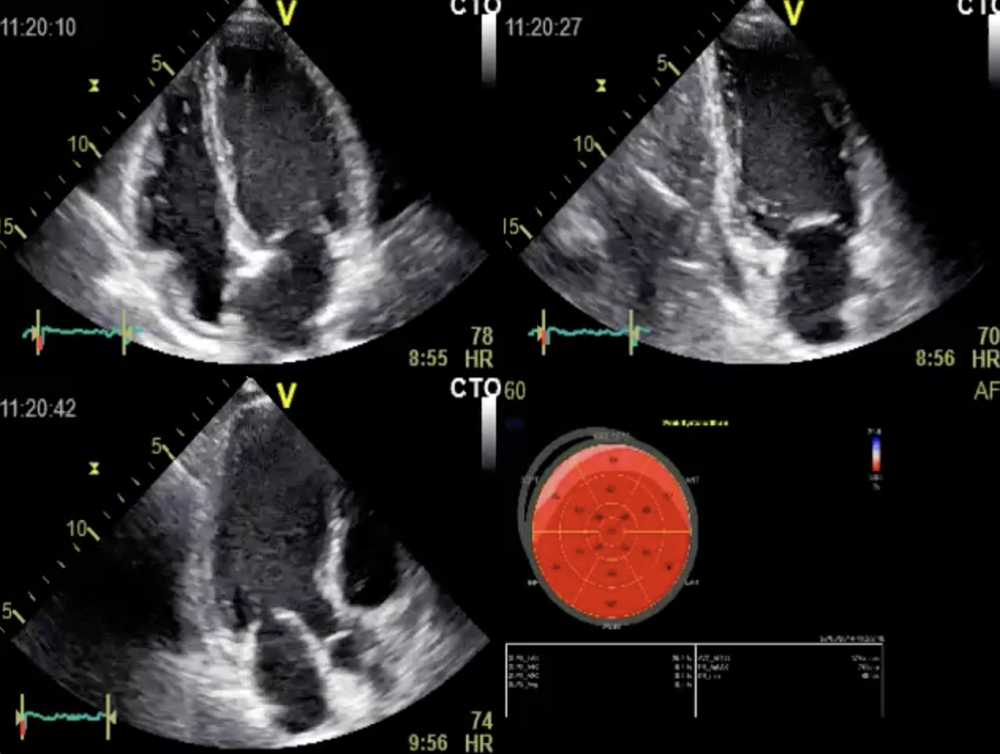 Normal global longitudinal strain (GLPSS) of – 19.2%. The patient has normal longitudinal function.
Normal global longitudinal strain (GLPSS) of – 19.2%. The patient has normal longitudinal function.
Tip 5: Look at diastolic function
Look at diastolic function. If the patient has a very tall E wave relative to the A wave (E/A ratio is > 2) then you can be pretty sure left ventricular function (LVF) is normal (exception patients with restrictive CMP, patients with severe forms of LV dysfunction and transplant patients). Such patients actually have a super normal (diastolic) function. Remember, all patients with systolic dysfunction also have some degree of diastolic dysfunction. So normal diastolic function will help you to exclude systolic dysfunction.
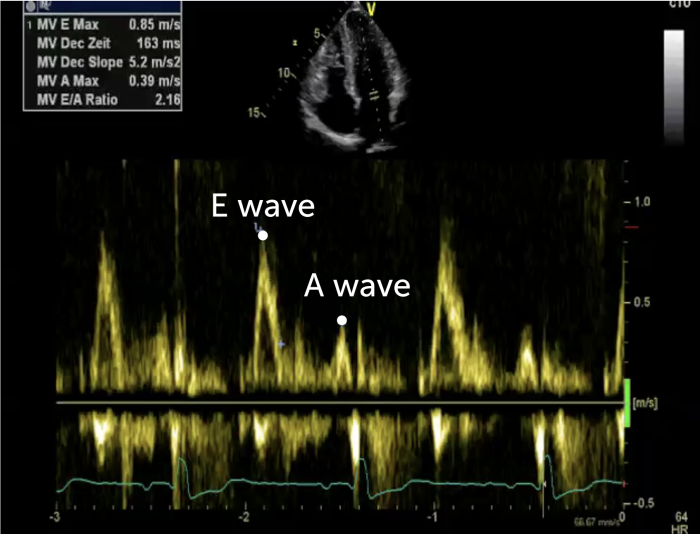 Mitral inflow signal with an E/A ratio of 2.2 typical for super normal filling. This finding practically excludes left ventricular dysfunction
Mitral inflow signal with an E/A ratio of 2.2 typical for super normal filling. This finding practically excludes left ventricular dysfunction
.. and pssssssst on a side note: If you are still not sure check the natriuretic peptides...
PS: If you have any questions you would like to have answered in one of my next posts – keep them coming...
Best
Thomas