
GI bleeding and Syncope – Can you spot the diagnosis?


A 70-year-old man presented to the emergency department with malaise, exertional dyspnea, and melena. He also reported one episode of syncope in the past week.
Lab: Hemoglobin: 10 g/dL (normal: 13–17 g/dL), Platelet count: 190 Tsd./µL (normal: 150–400 Tsd./µL),...
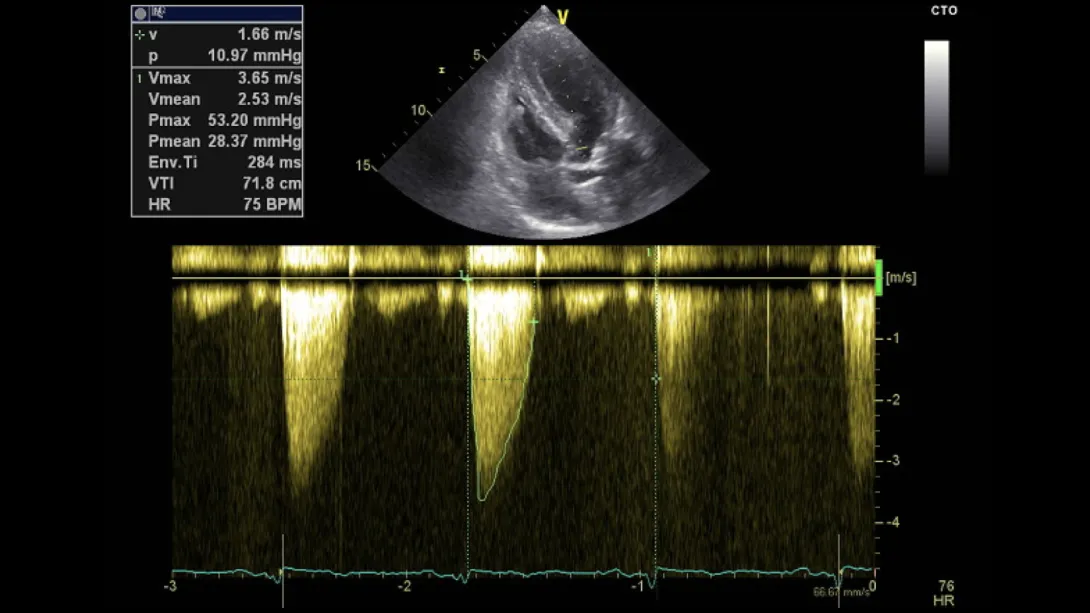
On the first day of admission, a transthoracic echocardiogram was performed: Have a look!
What Are Your Thoughts?
Based on the clinical presentation, laboratory findings, and echocardiographic imaging, what is your most likely diagnosis?
What additional exams would you perform in this patient?
What would be your treatment strategy for the diagnosis you made?
If you want to learn how to solve that case easily and quickly, then you should check out our newly launched Aortic Valve Disease FocusClass for our amazing launch offer!
Outcome:
Further investigations included an upper gastrointestinal (GI) endoscopy, which identified a proximal jejunal arteriovenous malformation (AVM), also known as a Dieulafoy lesion.
The combination of lower GI bleeding (angiodysplasia) and the presence of aortic stenosis on the echocardiogram led to a diagnosis of Heyde syndrome.
Although the patient’s aortic stenosis was not severe (Vmax (3.65 m/s) and Vmean (28.37 mmHg), moderate AS), the clinical correlation between the GI bleeding and the valvular pathology necessitated transcatheter aortic valve replacement (TAVR) to address the underlying cause.
Clinical Course:
After receiving a new aortic valve via TAVR:
- The patient’s bleeding resolved completely.
- Haemoglobin levels normalized over time.
- Episodes of syncope ceased.
Some explanations about the Heyde syndrome:
Acquired aortic valve stenosis develops due to atherosclerotic processes affecting the valve. Turbulent blood flow through the narrowed valve leads to shearing forces, which destroy von Willebrand factor (vWF), resulting in an acquired von Willebrand syndrome (type 2A).
Aortic valve stenosis can lead to left ventricular hypertrophy, manifesting as episodic syncope, dyspnea, and angina pectoris. Gastrointestinal bleeding can be either occult or present with visible blood in the stool, known as hematochezia. Vascular malformations primarily occur in the ascending colon and cecal regions. If angiodysplasia affects the more proximal parts of the gastrointestinal tract, additional symptoms such as hematemesis or melena may occur.
Symptomatic treatment for Heyde syndrome includes endoscopic management of gastrointestinal bleeding, pharmacological therapy (e.g., octreotide or antifibrinolytics), iron supplementation, blood transfusions and von Willebrand factor replacement, though definitive resolution typically requires addressing the aortic stenosis through transcatheter aortic valve replacement (TAVR) or surgical aortic valve replacement (SAVR)
Our patient case illustrates that TAVR can be the primary and definitive treatment. After valve replacement, the likelihood of bleeding generally decreases, and often no further treatment is needed.
Did you make the correct diagnosis? If you are still having difficulties, our newest course Aortic Valve Disease FocusClass will provide you with more information, cases, and patient demonstrations. Check it out now – and benefit from -30% and Lifetime Access!
Related Courses
The Aortic Valve Disease FocusClass offers a comprehensive overview of diagnosing and managing…

The Echo MasterClass is the most comprehensive premium online course in echocardiography,…