
Adult Congenital Heart Disease BachelorClass Case
Here’s a case from our Adult Congenital Heart Disease BachelorClass: A 60 y/o woman with palpitations and no relevant previous medical history presents at your echocardiography lab. She has tachycardia (around 150 bpm). In addition to the sensation of palpitations, she reports some dizziness and shortness of breath.
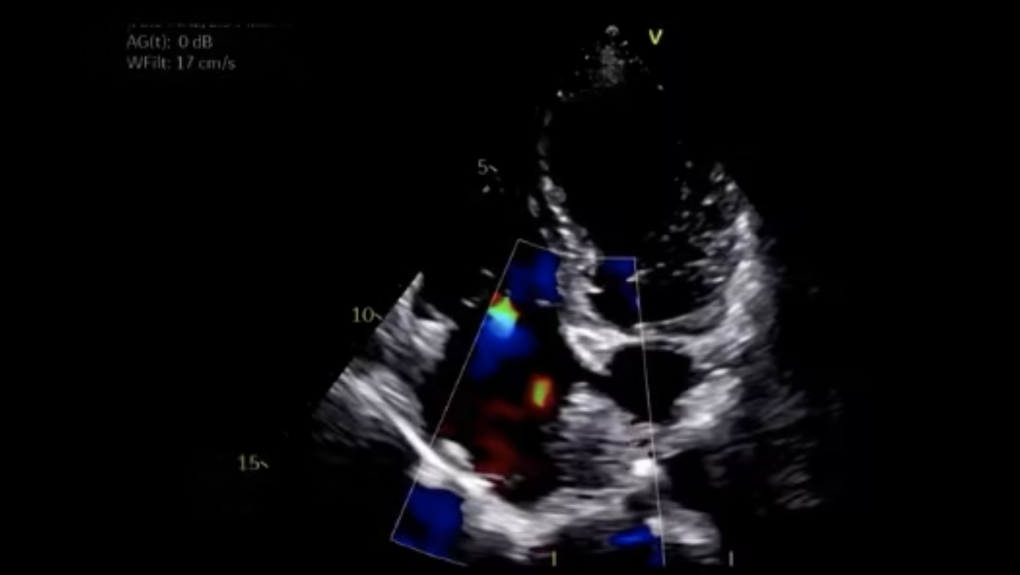
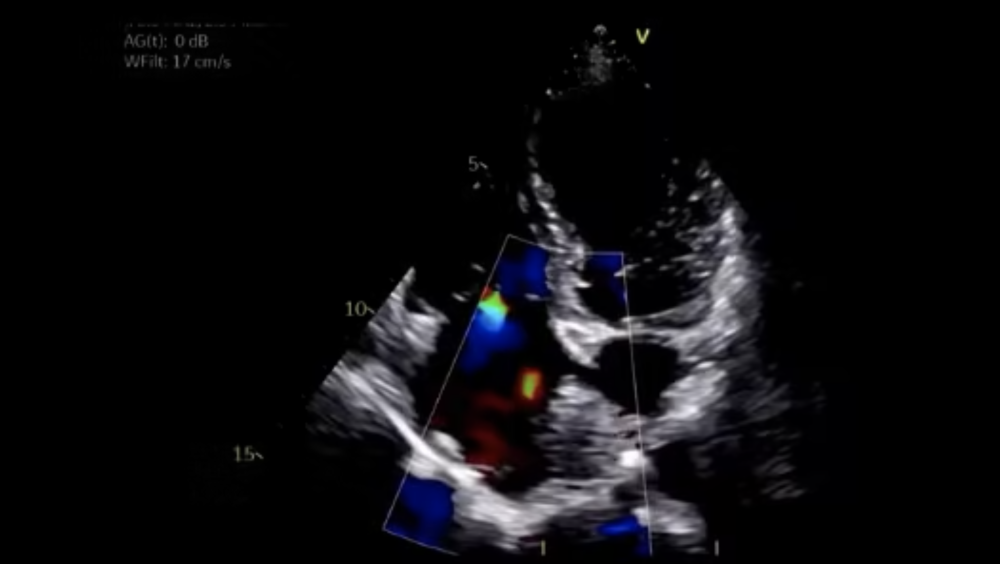
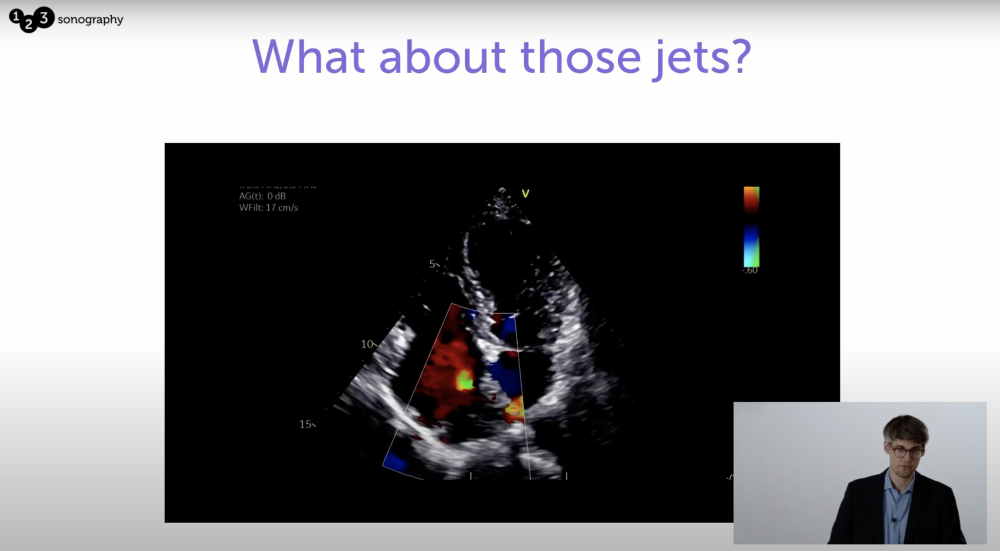
Where are these jets coming from?
Here is an A4C-view of this patient. You certainly spot the two quite peculiar looking jets – Where are they coming from?
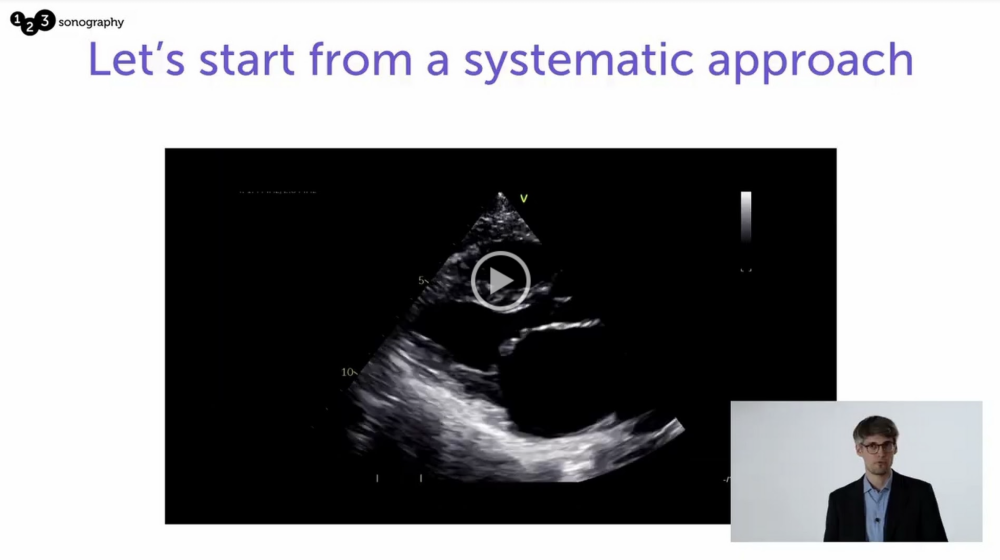
Before answering this question we go through this case systematically starting with a parasternal long axis (PLAX) view:
Is there anything that catches your attention?
Now let's move on to the parasternal short axis view (PSAX):
One, two, three?
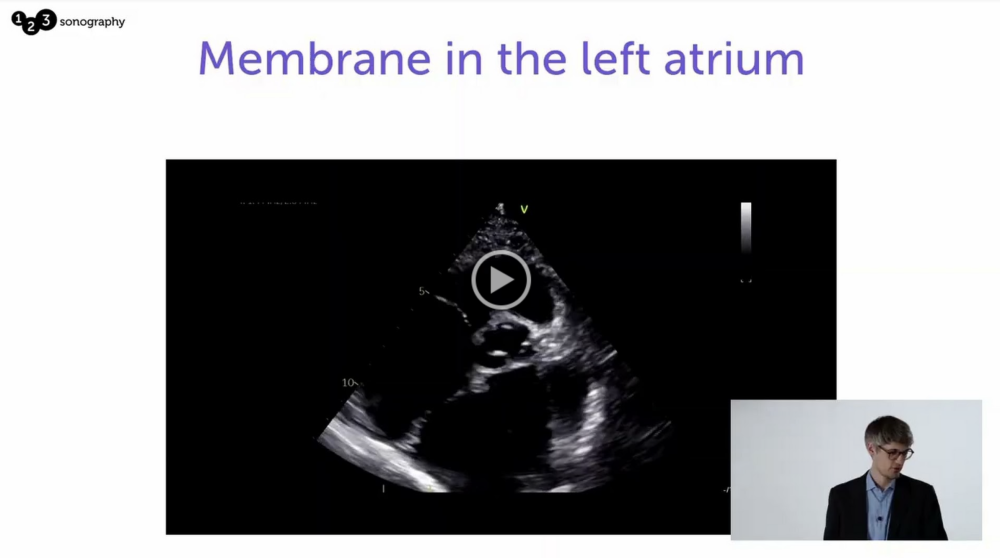
The apical 4-chamber view shows an even more impressive picture: In fact, this is not a 4-chamber but rather 5-chamber view because apparently, this patient has three atria!
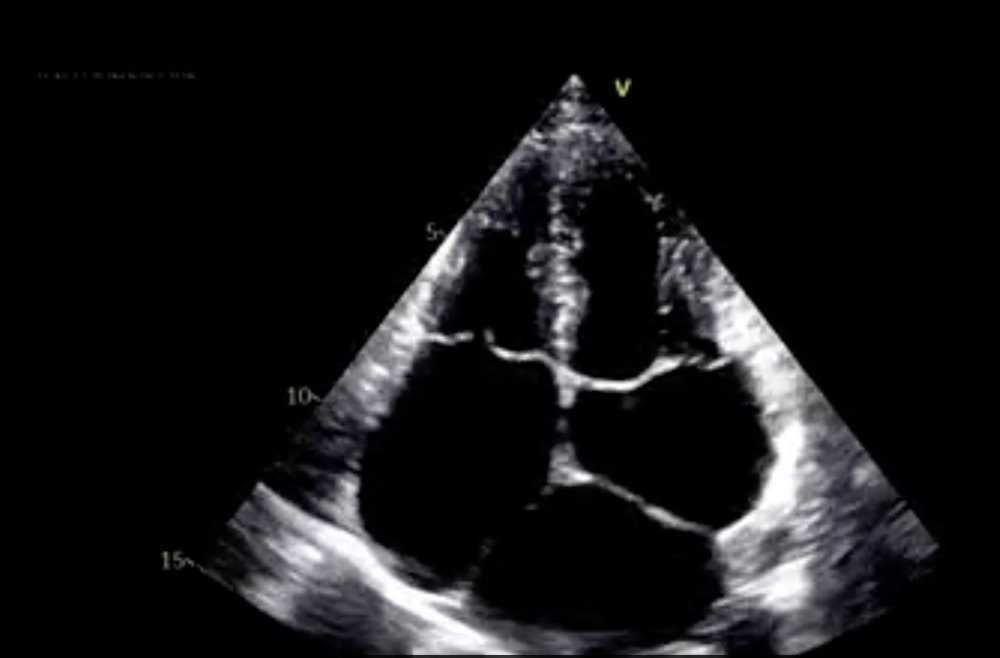
What’s the diagnosis?
Cor triatriatum sinister (CTS): This patient has two left atria!
Let us briefly discuss the anatomical features of the most common form of cor triatriatum sinister in which all four pulmonary veins drain into the proximal (superior) atrial chamber. Other more rare variants do exist but they are clearly beyond the scope here!
First, there is the distal (inferior) atrium, which is the "true" atrium. It is connected to the atrioventricular valve and contains the atrial appendage. The "true" atrial septum separates it from the right atrium, while the fibromuscular membrane separates it from a second chamber that is located proximal (or superior to it). The latter drains the blood from the pulmonary veins and has no direct connection to the mitral valve.
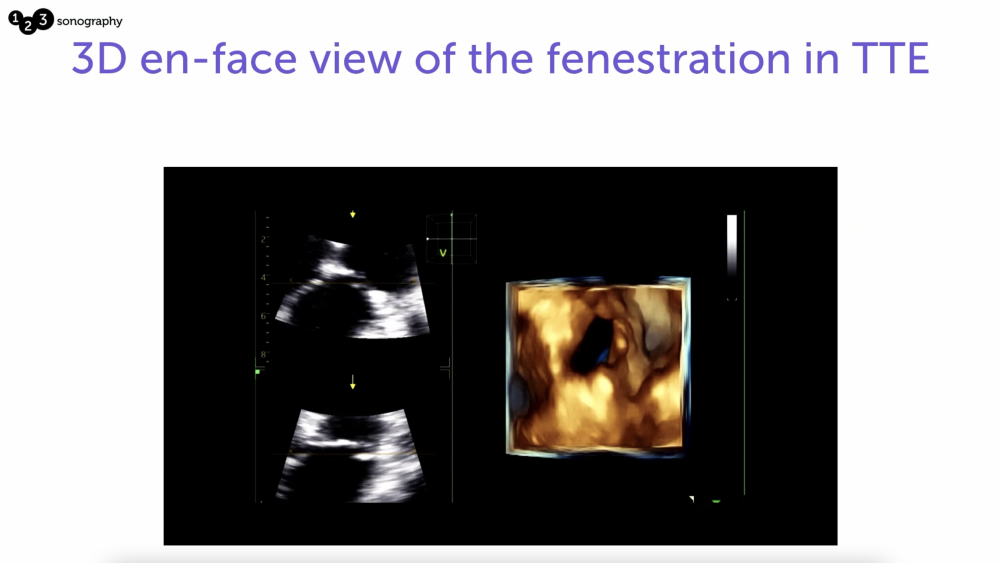
The membrane between the two chambers may be incomplete or fenestrated, sometimes enabling nearly unobstructed blood flow from the proximal to the distal chamber. In such cases, patients may have only mild or no symptoms, which is why the diagnosis may only be made in adulthood or even post-mortem.
So, what does this diagnosis mean for the patient?
Well, it depends! There are all sorts of variations – as mentioned above, the hemodynamic significance of the flow obstruction and thus the severity of the symptoms depend very much on the continuity of the membrane! The constellation of symptoms typically mimic mitral stenosis: pulmonary hypertension, pulmonary edema (with dyspnea), cardiac arrhythmias, congestive heart failure, etc.! What we really need to find out is if there is a hemodynamically relevant stenosis!
Now let’s go back to our initial question: What about these jets?
This case illustrates nicely that, on the one hand, how late congenital heart disease may be diagnosed and, on the other hand, that they not only present in adult congenital heart disease clinics but may show up, although very rarely, in the midst of a routine echocardiography in any cardiology practice!
Get our Adult Congenital Heart Disease BachelorClass to learn more through cases like this one!