
Getting Closer to Our Patients' (posterior) Hearts

Transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) are two key echocardiographic techniques for visualising the heart. TTE is typically the first-line choice, but when might we need to get closer with TEE?
1. Settings and Equipment
TTE can be performed in diverse settings, including outpatient clinics, at the bedside, and in emergency departments. Portable TTE equipment, even handheld devices, allows easy access in various situations. Larger ultrasound machines are also mobile, typically equipped with multiple transducers for different scanning needs, including cardiac and abdominal imaging.
TEE, on the other hand, requires a controlled setting, such as a procedure room or operating room. The equipment involves a flexible endoscope with a transducer at its tip for imaging the heart via the esophagus. TEE is more complex, requiring patient preparation, sedation, and additional personnel, making it semi-invasive and inherently more resource-intensive.
2. Technique and Limitations
TTE involves placing an ultrasound probe on the chest wall to capture images through specific acoustic windows, such as the intercostal spaces and subxiphoid areas. This non-invasive approach doesn’t require sedation, making it simpler and faster, especially in emergency settings. However, the rib cage and lungs can limit image quality, even in skilled hands.

TEE offers a closer view by positioning the transducer within the esophagus, directly behind the heart. This proximity bypasses chest wall and lung interference, yielding high-resolution images. However, TEE’s semi-invasive nature means it requires sedation and has associated risks, so significant diagnostic benefits must justify it.
3. Indications
TTE is generally the first choice for evaluating ventricular function, valve structures, and pericardial effusion, and is well-suited for routine exams and stable patients.
TEE is ideal for high-detail imaging, especially for posterior heart structures that are difficult to visualize with TTE. Indications include suspected endocarditis, cardiac masses, prosthetic valve assessments, and intraoperative monitoring. It’s invaluable in critical care for real-time, high-resolution imaging.
4. Diagnostic Value
TEE provides superior visualisation of posterior cardiac structures (e.g., atria, mitral valve, pulmonary veins) due to the close proximity of the esophagus to these areas. High-frequency transducers can be used, offering better spatial resolution, crucial for diagnosing intracardiac masses, thrombi, or small vegetations on valves. In cases like infective endocarditis or atrial appendage thrombus, TEE can provide critical details that TTE may miss due to body habitus or lung interference.
Case Example:
A 70-year-old male with a bileaflet mechanical mitral valve presents with worsening dyspnea.
TTE Findings:

Elevated left ventricular inflow velocity, turbulent flow directed toward the interventricular septum, and an enlarged left atrium suggest possible valve obstruction. However, direct visualization of the leaflet function is limited on TTE, making TEE necessary for further evaluation.
TEE Findings:
On closer inspection in a TEE study, one of the occluders appears to be stuck and immobile, and there is also a thrombus in the same area. This thrombus is the reason why the occluder is stuck. This condition is known as thrombotic mechanical mitral valve obstruction! Keep in mind, that the differentiation between thrombus and pannus is crucial for subsequent treatment! - stronger anticoagulation treatment and thrombolysis can dissolve a thrombus. A pannus, being fibrous tissue rather than a clot, does not respond to anticoagulation or thrombolytic therapy!
5. Cost Considerations
TTE is more cost-effective due to its minimal equipment needs and lack of requirement for sedation or specialized personnel, making it suitable for routine cardiac assessments. TEE, with its additional equipment and sedation requirements, is inherently more costly and therefore used selectively.
6. Risk Considerations
TTE is non-invasive, painless, and generally risk-free. TEE, however, carries greater risks due to its semi-invasive nature. Possible complications include esophageal trauma, aspiration, and sedation-related reactions, making pre-procedure fasting and patient monitoring essential.
7. Take-Home Message
TTE is the preferred method for routine cardiac assessments: safe, accessible, and cost-effective. It often answers the question, “What’s going on?” TEE, however, is reserved for cases requiring detailed imaging of specific structures, especially when TTE results are inconclusive or high-resolution imaging is essential, such as during surgery. It can answer questions like, “Which structures are involved?” and “What does the pathology look like in detail?”
In summary, both TTE and TEE play essential roles in echocardiography. TTE serves as the accessible, first-line diagnostic tool, while TEE offers enhanced imaging for complex cases.
Interested in advancing your skills? Join our TEE MasterClass now and save 40%!
Another case example:
72-year-old male with Atrial fibrillation (AF) coming for elective cardioversion (persistent AF symptoms).
TTE:
There is a strong suspicion of a Thrombus in the left atrium / left atrial appendage region. LAA visualisation is poor on TTE (also because of the patient's habitus). TEE is recommended to evaluate thrombus mobility, size, and morphology, which are critical in assessing the embolic risk, especially for high-risk procedures, like cardioversion.
TEE Findings

Large, mobile, "pear-shaped" thrombus in LAA; protruding toward mitral annulus. High embolic risk due to mobility and size, plus patient’s poor left ventricular function and left atrial enlargement. Anticoagulation is intensified to reduce thrombus risk pre-cardioversion. And the Cardioversion is postponed until thrombus resolution! A follow-up TEE is planned.
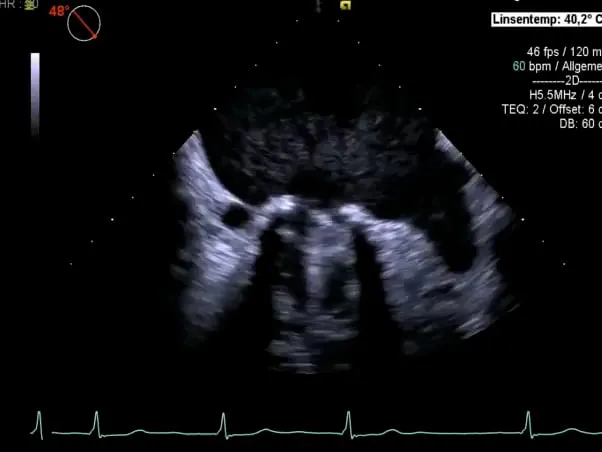
Last but not least:
TTE can sometimes show thrombus formations with extremely good resolution as in this example of a thrombus in the apex, as this region lies quite close to the transducer!

Related Courses

The TEE MasterClass is an exclusive teaching program that will allow you to learn the art of…