3.3.2 Right ventricular size
Owing to its complex geometry the right ventricle is difficult to measure. However, even if measurements are less exact and correlate modestly with calculations of size performed with cardiac magnetic resonance imaging (CMR), it is still important to quantify the right ventricle with echo. Right ventricular enlargement always is a pathologic finding; the investigator must search for, and identify the reason.
Always search for the cause of RV dilatation.Potential reasons are listed in the following table:
Causes of RV Dilatation Dilated Cardiomyopathy Myocarditis Right ventricular dysplasia Right heart infarction Pulmonary embolism Pulmonary hypertension Atrial septal defect Tricuspid regurgitation Pulmonic regurgitationCompare the right ventricle and the left ventricle. This can also be done by visual assessment. The left ventricle is usually at least thirty percent larger than the right one.
In severe forms of RV dilatation, the apex of the heart is formed by the right ventricle instead of the left one.
The size of the right ventricle can be determined either with 2D measurements, area or volume calculations. MMode measurements were used at the beginning of echocardiography (parasternal axis). However, as these measurements are very inexact and strongly depend on how the Mode "cuts" through the right ventricle, they are no longer used. It is far better to measure distances in 2D. This is best done on an optimized 4-chamber view or a subcostal view at end-diastole. Roughly, the ventricle appears triangular on these views. Thus the diameter varies, depending on the level at which the measurements are performed.
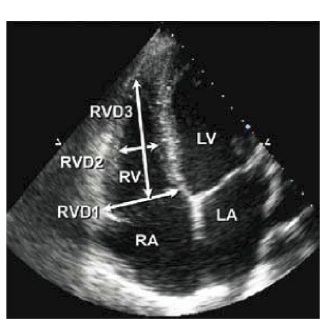
Two sites are commonly used: the basal distance (at the tricuspid annulus) and the mid-right-ventricular measurement (in the middle segment of the RV). The length of the right ventricle is less frequently used. Normal values are given in the following table:
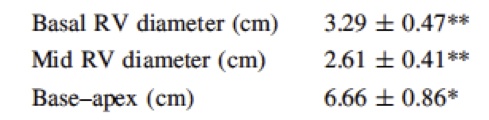
Roughly, a mid-right-ventricular diameter of 35 to 40 mm or 42 to 45 mm at the base indicates right ventricular dilatation. Respiration influences the size of the right ventricle. During inspiration it is slightly larger. It is important to take the patient's body surface area into account.
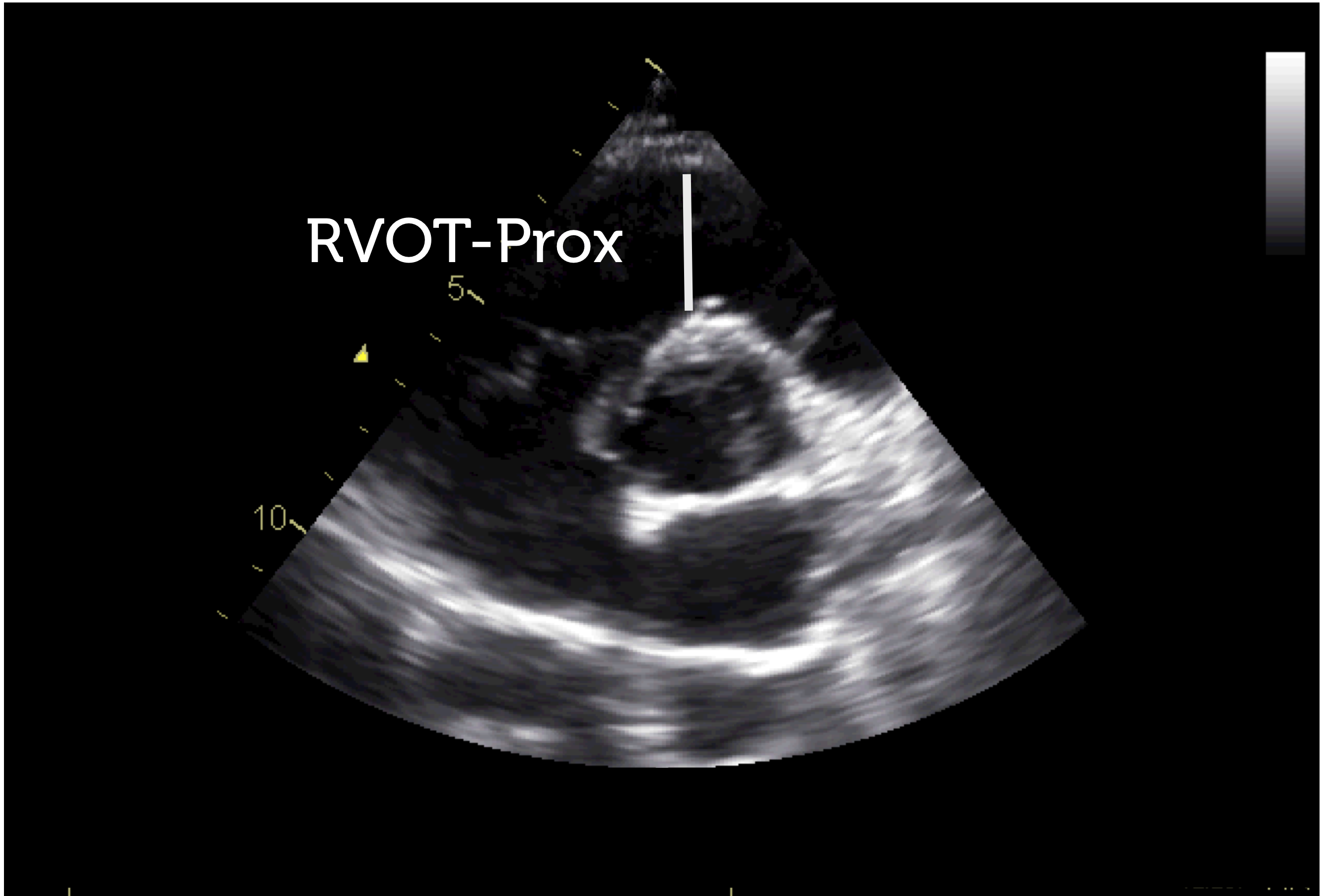
An apical transducer position that is too high will lead to overestimation of RV sizeIt is also possible to measure the width of the RVOT on a parasternal short axis view at the base. Here the upper limit of normal is 33 mm for the proximal aspect and 27 mm for the distal aspect at the level of the pulmonary valve.
Several methods have been proposed for quantification of right ventricular function. The most relevant techniques are presented in this section. Obviously you will not need to perform them all, but use at least use one or two, especially in patients in whom right ventricular function is very important. Also consider the fact that echo is by far less accurate than cardiac magnetic resonance imaging (CMR), which may be regarded as the gold standard.
CMR is the gold standard for quantification of right ventricular function. However, this method also has limitations.