
Acute appendicitis II

Case Presentation
A 19 year old girl presents with acute pain in the right lower quadrant followed by nausea of 4 hours duration. Laboratory findings reveal mild leukocytosis, and her B-HCG titer is negative.
 Caption: Sagittal sonogram of the right lower quadrant. | Description: Sagittal sonogram reveals a tubular, hypoechoic non-compressible structure at the site of maximal tenderness. It measures 11 mm in maximum dimension and contains a linear echogenic mass with posterior shadowing measuring 1.4 cm.
Caption: Sagittal sonogram of the right lower quadrant. | Description: Sagittal sonogram reveals a tubular, hypoechoic non-compressible structure at the site of maximal tenderness. It measures 11 mm in maximum dimension and contains a linear echogenic mass with posterior shadowing measuring 1.4 cm.
First published on SonoWorld
 Caption: Transverse sonogram at the site of maximal tendern | Description: Transverse sonogram demonstrating the echogenic focus within the tubular structure.
Caption: Transverse sonogram at the site of maximal tendern | Description: Transverse sonogram demonstrating the echogenic focus within the tubular structure.
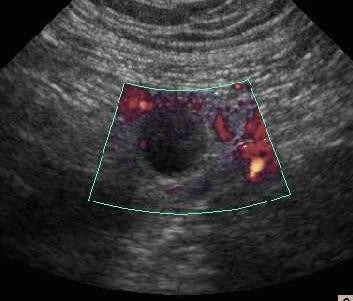 Caption: Power Doppler study of the right lower quadrant. | Description: Power Doppler view of the tubular structure demonstrates no flow within the lumen; however, minimal vascularity is noted in the surrounding wall.
Caption: Power Doppler study of the right lower quadrant. | Description: Power Doppler view of the tubular structure demonstrates no flow within the lumen; however, minimal vascularity is noted in the surrounding wall.
Differential Diagnosis
Acute appendicitis with appendicolith.
A dilated ureter with calculus [unlikely as the calcific focus is cephalad to the dilated tubular structure]
Final Diagnosis
Acute appendicitis with an obstructing appendicolith.
Discussion
Acute appendicitis can be catastrophic if timely intervention is not provided. Many studies worldwide have regarded ultrasound as a reliable imaging modality to not only diagnose appendicitis and its ensuing complications, but also provide an alternative differential diagnosis, if need be. Some studies have shown comparable accuracy when comparing ultrasound to unenhanced helical CT scan, and therefore ultrasound is often employed due to its cost effective nature and easy portability.
Graded compression ultrasonography is the technique used to visualize the appendix. The proposed radiologic criteria to diagnose non-perforated acute appendicitis include visualization of a non-compressible, aperistaltic appendix with an outer diameter of 6 mm or more. A target appearance of the appendix may be seen in the transverse view. Peri-appendiceal fluid and appendicoliths may also be noted. The appendicoliths commonly obstruct the lumen of the appendix as is seen in our case, and trigger the inflammation. Enhanced vascularity demonstrated by color Doppler in the wall of the appendix may support the diagnosis. A complex cystic mass in the right iliac fossa may be seen if an appendicular abscess forms. In cases with a high index of clinical suspicion for a perforated appendix, presence of loculated pericecal fluid even in the absence of visualization of the appendix should raise concern for the diagnosis, however other etiologies which could result in a similar appearance, such as perforated right sided diverticulitis, would have to be excluded and CT scan may be necessary then.
Han, et al reported the utility of a saline enema to aid visualization in the pediatric patient. Sometimes however, technical factors, such as obese or muscular patients, a deeply located appendix and lack of operator expertise, may hinder the visualization of the inflamed appendix. In such circumstances and in patients with atypical presentations, an alternative modality, usually CT, is performed.
Follow Up
This patient underwent an emergent appendectomy and an acutely inflamed appendix was removed at surgery.
Case References
1.Poortman P, et al. Comparison of CT and USG in the diagnosis of acute appendicitis: a blinded prospective study. AJR. 2003 Nov; 181(5): 1355-9. 2.Vegar-Zubovic S, et al. Ultrasound in the diagnosis and differential diagnosis of acute appendicitis in childhood. Med Arh. 2003; 57(4): 233-6.
3.Jeffrey RB Jr, et al. Acute appendicitis: sonographic criteria based on 250 cases. Radiology. 1988 May 167(2): 327-9.
4.Borushok KF, et al. Sonographic diagnosis of perforation in patients with acute appendicitis. AJR. 1990 Feb; 154(2): 275-8.
5.Quillin SP, Siegel MJ. Diagnosis of appendiceal abscess in children with acute appendicitis: value of color Doppler sonography. AJR. 1995 May 164(5): 1251-4.
6.Han TI. Improved sonographic visualization of the appendix with a saline enema in children with suspected appendicitis. J Ultrasound Med. 2002 May 21(5): 511-6.